Arcadia Health Solutions is a population health company that helps providers and insurers in their transition to a value-based care model. Arcadia is working with several of the Blues, Cigna, Beth Israel, and more. While it started as a consulting firm, in recent years Arcadia has raised over $40m from Merck, GE, and other corporate venture funds.
Listen to Matthew Holt’s interview with Sean Carroll, CEO of Arcadia Health below.
Part 2 picks up where Part 1 left off, as coincidence would have it.
Soeren Mattke (as mentioned in the last installment) and I were quite relentless in trying, quixotically, to get Professor Baicker to explain her results. Its popularity could have landed her many profitable speaking and consulting gigs, but she evinced no interest in cashing in, or even in defending her position. Indeed, the four times she spoke publicly on the topic, she didn’t do herself, or her legions of sycophants in the wellness industry, any favors. In each interview, she distanced herself more and more from her previous conclusion. Here are her four takeaways from her own study “proving” wellness has precisely a 3.27-to-1 ROI:
Individually or in total, these comments sounded an awful lot like retractions, but she (and her co-author and instigator, David Cutler) claimed those comments didn’t constitute retractions. Whatever they were, she wasn’t exactly doubling down on this 3.27-to-1 conclusion.
Here’s where it gets interesting. Due to this relentless criticism, instigated and sometimes written by me (most of which is catalogued here) with credit to Soeren Mattke and Jon Robison as well (with Pulitzer Prize-winningLA Times columnist Michael Hiltzik piling on multiple times), Ron Goetzel and his colleagues urged Professor Baicker — who had previously claimed to have no more interest in wellness — to get a grant from Ron’s friends at the Robert Wood Johnson Foundation and do an actual controlled study of workplace wellness to set the record straight. As a strategic gambit, this showed a level of professional judgment worthy of Gary Hart.*
He even forged a letter from the governor of Nebraska to cover his tracks. (To be completely accurate, he did not forge the signature on the letter. He merely doctored the wording in a letter that was already signed to say something much different than the letter said when it was actually signed. Maybe that’s not technically forgery. Who knows?)
And yet that’s exactly what Mr. Goetzel did. Maybe he thought she was as corrupt as he is, but she has an excellent reputation in this industry. My suspicion is that she accepted his offer for exactly the opposite reason that he made it — to clear her name after her ill-considered 2010 meta-analysis.
Where does the wellness industry go from here? They’re hoping for Tiger Woods, wiser souls are channeling Gary Hart, and probably what we’ll get instead is Harold Stassen. (Look it up.)
*For those of you who aren’t old enough to remember, here’s what happened. Dogged by rumors of philandering, the front-running Democratic presidential candidate urged reporters to follow him around. It took about a day for reporters to discover he was indeed philandering. It only took another few weeks for him to withdraw from the presidential race.
Al Lewis, the originator of risk-based population health contracting and outcomes measurement, is founder and President of the Disease Management Purchasing Consortium International, Inc. This article originally appeared on Dismgmt here.
Let’s climb into the WABAC Machine (and, yes, that’s the way it’s spelled) and set the dial for 2008.
Then-candidate Barack Obama, campaigning on the promise of universal health coverage, enlisted Harvard professor David Cutler as his key adviser on that topic. Business lobbying associations were not thrilled about their members having to cover all their full-time employees and incorrectly assumed, then as now, that the major drivers of healthcare cost were employees smoking, overeating, and not exercising. Prof. Cutler suggested, quite correctly, that one way to assuage that concern would be to allow employers to spend less money covering employees with those three health habits.
Fast-forward to 2009, when it appeared that — with enough concessions to enough vested interests — the Affordable Care Act (ACA) could become a reality. Business lobbying groups were, then as now, powerful entities. Using Prof. Cutler’s suggestion, they were pacified by allowing businesses to tie up to 30% of total premium dollars to employee health (in practice, largely employee weight). Generally, the business lobbying groups engineered this withhold in the shadows. It wasn’t until 2015 that one of those business groups, the Business Roundtable, publicly admitted that the 30% withholdwas the main reason they bought into the ACA.
What the Administration needed in addition to the Safeway experience was some academic support. It happens there is an old joke among economists that the definition of “economist” is someone who, upon finding that something works in practice, wonders whether it will work in theory. Enter Professor Cutler again. He enlisted the then-little-known Katherine Baicker, of the Harvard School of Public Health, who had no background or apparent interest in wellness, to lead-author a meta-analysis to prove that wellness works (he was the second author).
She “proved” the theory that wellness works by citing basically every research study ever published. In those days, like today, essentially every published study — virtually all published by wellness promoters in wellness trade journals — showed savings, thanks to three rather transparent fabrications:
Looking only at the decline in high-risk members and not the increase in risk by the low-risk members
Drawing a trendline straight up and saying how much cost was “avoided” because expenses didn’t rise that fast.
The resulting meta-analysis, Workplace Wellness Programs Can Generate Savings, was raced into publication in Health Affairs, peer review be damned. (Indeed it was published so quickly that Prof. Cutler didn’t have time to disclose his conflict of interest.)
The finding was quite definitive, to two significant digits: wellness produced a 3.27-to-1 ROI on cost savings alone. This is an almost unheard-of level of precision and conclusiveness in a population health analysis. Plus, an additional precise 2.73-to-1 on productivity.
The game was supposed to be over. That article was supposed to be the cherry on top of the ACA, academically blessing the one aspect of ACA which both parties supported. It was billed as a true win-win, saving money by getting employees to be healthier. This article became the single most influential article in Health Affairs history, with 935 academic citations alone, plus an untold number of start-ups, corporate program implementations, and references in lay publications.
Part 2 will cover how Prof. Baicker distanced herself from this result to the point of disowning it…and how withering criticism from myself and others (notably The Incidental Economist) created a chain of events which got her back in the game despite saying she had “no interest.”
Al Lewis, the originator of risk-based population health contracting and outcomes measurement, is founder and President of the Disease Management Purchasing Consortium International, Inc. This article originally appeared on Dismgmt here.
Today, we’ve got another episode of Health in 2 Point 00—airport edition. On Episode 78, Jess is spending the last few moments before her vacation interviewing me from the airport. She asks me about lots of big raises: Redox raised $33 million for their interoperability platform; EverlyWell, which offers direct-to-consumer lab testing, raised $50 million, and Ro raised another $85 million just a year after raising $88 million. In other news, SureScripts is getting sued by the FDIC for monopolizing the e-prescriptions market and the FBI just raided uBiome for double-billing insurers. —Matthew Holt
Fifteen years ago, as a medical student, I learned a
terrifying lesson about blindly using race-based medicine. I was taking care of
Mr. Smith, a thin man in his late 60s, who entered the hospital with severe
back pain and a fever. As the student on the hospital team, I spent over an
hour interviewing him, asking relevant questions about his medical and social history,
the medications he took, and the details of his symptoms. I learned Mr. Smith
was a veteran who ran into tough times that left him chronically homeless,
uninsured, and suffering from hypertension and diabetes. I performed a complete
physical exam, paying particularly close attention to his back. Upon reviewing
his blood tests and kidney function, I read the computer’s report: “normal.”
I felt confident as I presented Mr. Smith’s treatment plan
to my attending physician: I recommended a CT scan, ibuprofen for pain, blood
pressure lowering medication, and an antibiotic. My attending listened quietly,
reviewed the labs herself, and then firmly corrected every aspect of my
treatment proposal. “His kidney function is NOT normal. What you want to do for him can further damage his kidneys. The lab
reported his creatinine as ‘normal’ because it has an algorithm that makes
faulty assumptions based on race.” Mr. Smith, according to the medical record,
was African American.
I almost harmed Mr. Smith because I hadn’t realized that the exact same creatinine level (the key metric for kidney function) yields two different reports based on whether you’re African American or not. The logic goes that because black people supposedly have higher muscle mass on average, healthy creatinine levels for those who check the “black” box is different from those who check other boxes. Physicians around the country continue to rely on this metric even when the black patient is thin, like Mr. Smith. This example of race-based creatinine levels to determine kidney function is a symptom of race-based medicine in general: (poorly defined) racial categories are often used as proxies to explain discrepancies in health outcomes by race, which is a potentially dangerous analysis. Mr. Smith’s case forced me to consider why race-based medicine is problematic and where our attention as healthcare providers should be directed instead.
What is certain is that health inequities persist along racial lines. African Americans and Hispanics have higher rates of diabetes, hypertension, and heart disease than other groups (Figure 1).[1] American Indians and Alaskan Natives are 2.1 times as likely to be diagnosed with diabetes as white individuals and the prevalence of obesity in this population is higher than any other group. While it would be convenient to attribute these disparities to genetic difference, this is simply not the case.
Using race to predict different health outcomes is
problematic for more reasons than one. Let’s start with why it’s bad science
and bad medicine. Because racial categories have been socially constructed, the
definitions and qualifications for each race are dependent on location and time.
These racial categories have been proven time and time again to mean very little genetically, yet medicine continues to assume that innate biological difference among races explains racial disparities in health. Why would we test race to predict muscle mass to then predict kidney function when instead we can just test muscle mass to predict kidney function? That would avoid crude metrics like race and use more scientifically-justified criteria to predict health outcomes.
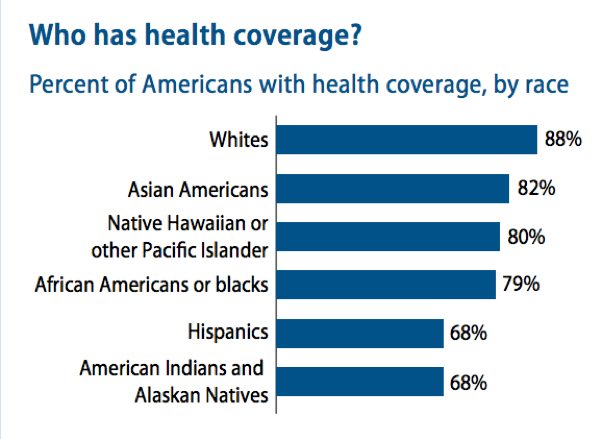
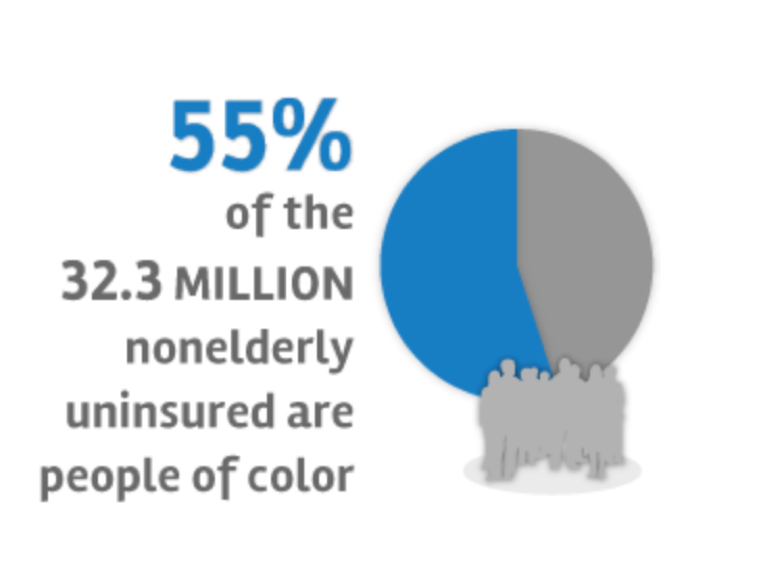
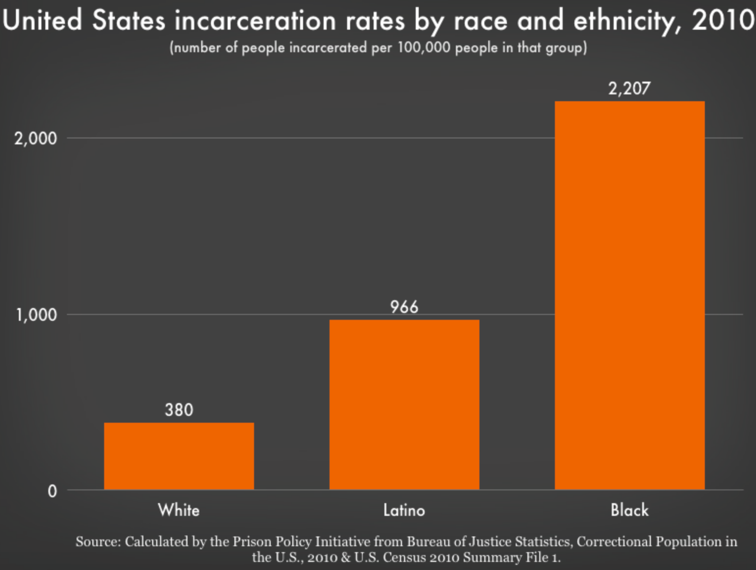
The second problem with race-based medicine is that it detracts clinicians from the social determinants of health disparities. If we really want to know why the above statistics hold true, let’s start by looking at insurance rates among these groups (Figures 2-3). Eighty-eight percent of whites have health insurance while only 79% of African Americans and 68% of Hispanics and Native Americans do. One in five Latinos reported not seeking medical care due to a language barrier. Forty-six percent of nonelderly blacks without health insurance report having one or more chronic health condition. High rates of incarceration among communities of color (Figure 4), exposure to environmental toxins, underfunded schools, food deserts, and the daily stress of racial discrimination all play powerful roles in determining health outcomes. Race-based discrimination also enters the hospital. Blacks and Latinos are twice as likely to be refused pain medication than whites for the exact same injury because black and brown patients are perceived to feel less pain or to somehow be more prone to addiction. These social and political factors, not race-based computer algorithms, must be the target of our focus as clinicians.
Figure 4. Source: Bureau of Justice Statistics.
As healthcare providers, we must focus on the much more complicated ways our country’s healthcare, education, and prison systems discriminately affect health outcomes. Thinking back to my experience with Mr. Smith, my plan should have addressed his homelessness and access to healthcare as causes for his sickness because for him, social factors, policies, and opportunities influenced his health far more than genetics. Mr. Smith’s case taught me a valuable lesson that I continue to believe today: when we see differences in health outcomes along racial lines, our focus should not be directed toward innate biological difference, but toward social inequity. The medical establishment, and we as healthcare providers, have a big role to play in changing this narrative.
Internist, Pediatrician, and Associate Professor at UCSF, Dr. Le is also the co-founder of two health equity organizations, the HEAL Initiative and Arc Health.
[1] The authors understand that the term “Hispanic” is controversial. We have decided to use this term in this instance, however, to be consistent with the categorizations used by national healthcare agencies, such as the CDC. For more discussion about on the term, see here.
Today THCB is spotlighting Lumeris which creates a platform to help set-up and develop health plans and manage care delivery for patients. Working with its associated medical group Essence, Lumeris has been creating actionable steps to reduce Medical Cost Rates (MCRs) and is now taking that process to other health systems that want to set up Medicare Advantage plans. Lumeris is working with 12 health systems and is growing rapidly. Recently, Lumeris partnered with Cerner to bring their product to market.
Matthew Holt interviewed Matt Cox, Chief Marketing Officer at Lumeris to find out the details.
In my mid-twenties, I was twice prescribed the common antihistamine
Benadryl for allergies. However, my body’s reaction to the drug was anything
but common. Instead of my hives fading, they erupted all over my body and my
arms filled with extra fluid until they were almost twice normal size. I subsequently
described my experience to a new allergist, who dismissed it as “coincidence.”
When I later became a nurse, I learned that seemingly “harmless” medications often cause harm, and older adults are particularly vulnerable. Every year, Americans over age 65 have preventable “adverse drug events” (ADEs) that lead to 280,000 hospital stays and nearly 5 million outpatient visits. The Lown Institute in Boston draws attention to this underrecognized problem in their recent report, Medication Overload: America’s Other Drug Problem. Policymakers, patients, and health professionals must act, because over the next decade, medication overload is predicted to cause 4.6 million hospitalizations of older Americans and 150,000 premature deaths.
Nearly half of all older adults take at least five
prescription drugs, a 300 percent increase from 25 years ago. The
more drugs we take, the likelier it is that one of them, or some combination,
will cause serious harm. When you add in non-prescription medications,
including over-the-counter drugs like ibuprofen and Tylenol, as well as
vitamins and herbal supplements, the potential for harm only goes up.
I’ve seen this in my
work. It is not unusual for elderly, very ill patients on hospice to have
prescriptions for 20 to 30 drugs. Several of their medications may treat the
same problem, amplifying any serious side effects. Blood pressure medications provide
a good example. As older patients become more debilitated, lose weight, and are
taxed by other health issues, the effect of these medications can intensify,
severely lowering blood pressure, and causing the patients to fall. Indeed, if
I am following up with a hospice patient who has fallen, the first thing I
check is their prescription medications for hypertension.
Given the prevalence of ADEs,
why are medications still prescribed so readily? We are all, patients and
prescribers, deeply embedded in a culture of prescribing, wedded to the idea
that all health problems can be solved by taking a pill, or a lot of pills. Clinicians also feel increasingly
pressured to hurry through appointments, and offering pills makes visits go
faster. For patients, receiving a prescription often gives them a sense of being
well-cared for.
Even clinicians who try to prescribe thoughtfully may feel pressure from patients who, having been enticed by drug advertisements to “ask their doctor” about a host of different medications, view a prescription as the key to better health. Direct-to-consumer drug advertising accelerated in 1997 when requirements for listing side effects were loosened by the FDA. That increase has coincided with a rapid rise in the rate of prescription drug use—and ADEs.
Most clinicians do not know how overloaded by medications their
patients are. Patients with multiple health problems likely receive
prescriptions from multiple specialists; no one doctor, nurse practitioner, or physician’s
assistant tracks and manages every drug a patient takes. Additionally, clinicians
are reluctant to discontinue medications because they worry that stopping a
prescription will cause harm.
Finally, physicians and other prescribers receive little to
no practical training in preventing medication overload or in deprescribing.
They may have learned that taking multiple medications can be a problem,
especially for older adults, but figuring out how best to avoid that problem
for individual patients is not easy. Consider warfarin, an anticoagulant and
one of the medications that often lands patients in the emergency department.
This drug is used routinely to prevent strokes from blood clots. It also
carries a risk of spontaneous bleeding and requires careful management to be
effective without being dangerous. For some older patients, aspirin will work
as well as warfarin, and would be much safer, but for other patients, the
reverse is true.
Medication overload is a tricky, multifaceted problem
without a simple solution. Over the past six months, the Lown Institute has
brought together a group of doctors, academics, pharmacists, nurses (including
myself), and patients to discuss what can be done.
Through our discussions, it has become clear that the best
way to reduce medication overload is for patients and prescribers to work
together. Patients need to understand that every drug has side effects, and
dangerous drug-to-drug interactions are always possible. Prescribers need more training
to help them recognize medication overload, and they need to be reimbursed for
the time it takes to talk over medications with patients. Clinicians and
patients need to discuss treatment options and the potential benefits and harms
of their medications, and that can’t all be done in a 10-minute visit.
Systemic changes are also needed to prevent medication
overload. Care coordination needs to include pharmacists and nurses as active
participants in medication review and deprescribing. Older
patients need a yearly “prescription check-up” to go over all their medications, and consider lowering the doses of, or even discontinuing,
some drugs.
Stopping dangerous prescribing, or overprescribing, will not be easy. A sense of need leads patients to request medications, and good intentions, usually, cause physicians to reach for the prescription pad. But the problem must be addressed to keep our patients as safe as possible. It begins by understanding that every pill has the potential to cause harm. Then we work together—patients, clinicians, and policymakers—to kick our overprescribing habit.
Theresa Brown, RN, is a clinical nurse, author of the New York Times bestseller The Shift: One Nurse, Twelve Hours, Four Patients’ Lives and is a frequent contributor to the New York Times.
By SAMYUKTA MULLANGI MD, MBA, DANIEL W. BERLAND MD, and SUSAN DORR GOOLD MD, MHSA, MA
Jenny, a woman in her twenties with morbid obesity (not her real name), had already been through multiple visits with specialists, primary care physicians (PCPs), and the emergency department (ED) for unexplained abdominal pain. A plethora of tests could not explain her suffering. Monthly visits with a consistent primary care physician also had little impact on her ED visits or her pain. Some clinicians had broached the diagnosis of functional abdominal pain related to her central adiposity, and recommended weight loss. This suggestion inevitably led her to become defensive and angry.
Though
our standard screen for safety at home had been completed long ago, I wanted to
probe further, knowing that many patients with obesity, chronic pain and other
chronic conditions have suffered an adverse childhood – or adulthood –
experience (ACE). Yet, I hesitated. Would a busy primary care setting offer enough
latitude for me to ask about a history of trauma when it can occur in so many
forms, in so many ways and at different times of life? Furthermore, suppose she
did report a history of trauma or adverse experience. What then? Would I be
able to help her?
Nonetheless,
I began: “Jenny, many patients with symptoms like yours have been abused,
either emotionally, physically, or sexually, or neglected in their past.
Sometimes they have suffered loss of a loved one, or experienced or witnessed
violence. Has anything like this ever happened to you?”
This
yielded our first breakthrough. Yes, she had experienced neglect, with parents
who were separated for much of her childhood, and then later divorced. She had
seen her father physically abuse her mother. With little parental oversight,
she had engaged in drug and alcohol use throughout her teenage years. But, she
wanted to be sure we understood that this was all behind her. She had gotten an
education, was in a committed relationship, and had a stable job as a teacher.
That part of her life was thankfully now closed.
But was it? Research demonstrates the incredible prevalence of ACEs and their association with illness and health risk behaviors even much later in life. In a groundbreaking 1998 study, almost two-thirds of close to 10,000 participants reported at least one ACE, and 12% reported having four or more. Compared to participants who reported no ACEs, individuals with 4 or more ACEs were more likely to have severe obesity (Odds ratio (OR)=1.6), depression (OR=4.6), and a previous suicide attempt (OR=12.2). Research also suggests that cumulative ACE exposure matters more than the type of ACE , with the association between multiple ACEs and disease onset following an additive pattern. Not surprisingly, traumatic adult experiences also affect health outcomes.Of particular relevance for Jenny, previous trauma increases the likelihood of unexplained gastrointestinal syndromes(OR = 1.75).
The
prevalence of ACEs and their influence on health provides strong rationale for
asking about trauma in the adult primary care setting. Primary care treats the
whole person, not just one organ system, and these relationships are ideally
characterized by care continuity and trust, so patients may feel more
comfortable disclosing painful or, in their eyes, shameful experiences, to
their PCP. Unlike in the pediatrics setting, however, there appears to be
under-recognition and under-treatment of trauma for adult patients.
Inquiring
about trauma confronts many challenges in the adult primary care setting,
especially a PCP’s extensive care responsibilities in a limited time frame. How
might primary care physicians ask about trauma in a way that is sensitive to
time demands, yet also open to the many forms and types of trauma? Experts
recommend using standardized instruments. Using a form, however, runs the risk
that patients may disclose an experience not addressed during the encounter, or
that they do not disclose traumatic experience due to lack of human interaction.
In our practice, we often use a general question about trauma so patients can
answer without specifics, if they prefer: “Many people have experienced some
kind of trauma in their lives. That could be living in a war zone, but it could
also be growing up with a parent who was abusive or had substance use disorder.
It could be experiencing or witnessing violence, or being bullied. Has anything
like that ever happened to you?” Then, if indicated, we can follow up with an
ACE questionnaire or other modality.
What
if patients resent such questions? What if patients perceive their physical
symptoms are being minimized? In Jenny’s case, raising the question later in
the relationship when some trust had been established may have made her more
open to disclose her history. On the other hand, if the question had been posed
routinely during her new patient past medical and social history, when we
routinely ask about sex and drugs, and she did disclose, this could have greatly informed her treatment, led to better
therapy, and avoided unnecessary, expensive and potentially harmful testing.
Like
other sensitive topics (death and dying, sex), PCPs, being human, may be
uncomfortable having such conversations. However, we suspect that the primary
reason why providers are reluctant to ask their patients about their history of
trauma is that, once uncovered, they wonder how they can help.
To truly transform into a trauma-informed primary care practice, it is not enough to simply ask about patients’ experiences with trauma. A comprehensive approach invests in trauma training, in the form of employee workgroups, lunch sessions, or coaches. Institutional investments in a robust mental health professional and social work team, particularly if co-located in primary care, can meet some of these patients’ needs. Perhaps providers, would be more likely to probe about a patient’s experience with trauma when they know that they have trained professionals available who can help treat the patient suffering from this history, and that patients can experience improvement.
Ideally,
every primary care practice would become and stay trauma-informed through such
comprehensive efforts. But absent such organizational change, what can adult
primary care practitioners do about adverse experiences’ impact on their
patients’ health and well-being? First, ask them. We who frequently and
routinely inquire about adverse experiences learn quickly how prevalent such
experiences are in patients with eating disorders, pain, chronic diseases like
diabetes, and mental illness; in other
words, most of our patients. Second, serve as external validation by telling
the patient that something bad happened
to you, and it is not your fault. Sexual
assault experiences in particular, even those experienced by children, often
create guilt. Third, let patients know how such experiences can contribute to
their obesity, their substance use disorder, or other symptoms and conditions,
and how treatment of those conditions requires an understanding of the impact
of that experience. Finally, and most obviously, patients with ACEs or
post-traumatic stress syndrome, or who have newly divulged a long-withheld
story of trauma, need psychotherapy, not psychoactive medications.
Jenny
was initially skeptical when we discussed the possibility that her adverse
childhood experiences may be impacting her in non-intuitive ways today – her
obesity, her abdominal pain. Though initially disbelieving, Jenny did agree to
engage in more talk therapy with a social worker. At last check, she had not
needed to visit the ED for over four months!
Acknowledgements: We thank Israel Liberzon, MD, Michigan Medicine, Sheila Marcus, MD, Michigan Medicine, Katherine Rosenblum, PhD, IMH-E, University of Michigan, and Marcia Valenstein, MD, MS, Michigan Medicine, for their helpful contributions, for which they received no compensation.
Samyukta Mullangi is a physician at New York-Presbyterian Hospital and health policy researcher at Weill Cornell Medicine, where she studies business model innovation in health care as it relates to the adoption of new technologies.
In this episode of Radiology Firing Line Podcast, I speak with Bishal Gyawali MD, PhD. Dr. Gyawali obtained his medical degree from Kathmandu. He received a scholarship to pursue a PhD in Japan. Dr. Gyawali’s work focuses on getting cheap and effective treatment to under developed parts of the world. Dr. Gyawali is an advocate for evidence-based medicine. He has published extensively in many high impact journals. He coined the term “cancer groundshot.” He was a research fellow at PORTAL. He is currently a scientist at the Queen’s University Cancer Research Institute in Kingston, Ontario.
Saurabh Jha is an associate editor of THCB and host of Radiology Firing Line Podcast of the Journal of American College of Radiology, sponsored by Healthcare Administrative Partner.
At its April 4, 2019 meeting, the staff of the
Medicare Payment Advisory Commission (MedPAC) asked the commission to discuss a
very strange proposal: Doctors who treat patients enrolled in Medicare’s
traditional fee-for-service (FFS) program must join an “accountable care
organization” (ACO) or give up their FFS Medicare practice. (The staff may have
meant to give hospitals the same Hobbesian choice, but that is not clear from the
transcript of the meeting.)
Here is how MedPAC staffer Eric Rollins laid out the
proposal:
Medicare would require all fee-for-service providers to participate in ACOs. The traditional fee-for-service program would no longer be an option. Providers would have to join ACOs to receive fee-for-service payments. Medicare would assign all beneficiaries to ACOs and would continue to pay claims for ACOs using standard fee-for-service rates. Beneficiaries could still enroll in MA [Medicare Advantage] plans. (p. 12 of the transcript)
The
first question that should have occurred to the commissioners was, Are ACOs
making any money? If they aren’t, there’s no point in discussing a policy that
assumes ACOs will flourish across the country.
But
only two of the 17 commissioners bothered to raise that issue. They asserted
that Medicare ACOs are saving little or no money. Those two commissioners – Paul
Ginsburg and commission Vice Chairman Jon Christianson – did not mince words.
Ginsburg said ACO savings were “slight” and called the proposal to push doctors
into ACOs “hollow” and premature. (pp. 62-63) Christianson was even more
critical. He said the proposal was “really audacious,” and that no “strong
evidence” existed to support the claim that ACOs “can reduce costs for the
Medicare program or improve quality.” (pp. 73-74) Ginsburg and Christianson are
correct – ACOs are not cutting Medicare’s costs when Medicare’s “shared
savings” payments to ACOs are taken into account, and what little evidence we
have on ACO overhead indicates CMS’s small shared savings payments are nowhere
near enough to cover that overhead.
But Ginsburg and Christianson might as well have been
talking to a wall. The other 15 commissioners had no comment. In fact, the
majority of them said ACOs are saving money for Medicare and endorsed further
consideration of the staff’s suggestion that doctors should have to choose
between joining an ACO or never again billing the FFS Medicare program.
The only other objection offered at the meeting came
from commissioner Marjorie Ginsburg. She noted that under the staff’s proposal beneficiaries
would have to enroll in an ACO (currently beneficiaries are assigned to one
without their knowledge), and they would have to suffer financial penalties if
they saw providers outside of their ACO. But, she warned, that will be “a
really hot-button issue and we have to be extremely careful in how we present
this going forward or we’re going to get hammered.” (p. 88) Yet even Ginsburg
said punishing doctors who didn’t join ACOs was worth further discussion.
Four
ACO programs, same results: No savings
As the table below indicates, the four ACO programs the Centers for Medicare and Medicaid Services (CMS) has established since 2005 have had almost no impact on Medicare spending. [1] The four programs have raised or lowered Medicare’s net spending by only a few tenths of a percent. Please note that three of the four programs – the Physician Group Practice (PGP) demonstration (which ran from 2005 to 2010), the Pioneer ACO demonstration (2012 to 2016), and Next Generation demonstration (it began in 2016) – exposed ACOs to two-sided risk, that is, to the risk of sharing losses as well as savings. Only the Medicare Shared Savings Program (MSSP), a permanent program that began in 2012, exposed ACOs only to upside risk (the chance to make money). I point this out because ACO proponents seek to excuse the poor performance of the MSSP by claiming MSSP ACOs are not exposed to downside risk (the risk of losing money). The best known proponent of this evidence-free explanation is probably Seema Verma, Trump’s CMS administrator. MedPAC also promotes this notion. But as the table indicates, exposure to downside risk makes little difference. The three two-sided-risk programs performed only a few tenths of a percent better than the MSSP has.
ACO proponents have not been happy with these results.
But rather than concede the ACO isn’t working, they have argued there is
something wrong with the way CMS measures ACO savings and losses. They say CMS’s
use of historical rather than concurrent control groups renders CMS’s estimates
of savings and losses inaccurate. If CMS would use concurrent controls, they say,
ACOs would look better.
I won’t get into the gory details of this claim. [2] All you really need to know is that research using concurrent controls produces the same underwhelming results – ACOs still save only a few tenths of a percent. For example, the study of the PGP demo that produced the measly three-tenths of a percent savings (see table above) used concurrent controls. Similarly, a study of the MSSP by J. Michael McWilliams using concurrent controls reported a seven-tenths-of-one-percent savings for 2013-2014 (my calculation based on data reported in Table 2, p. 1712), while the National Association of ACOs reported a three-tenths-of-a-percent savings for the MSSP for 2013-2015 (see slide 9 in this presentation by MedPAC staff at the commission’s January 2019 meeting).
No
margin, no mission
So if Medicare ACOs are breaking even for Medicare, or
are at best cutting Medicare’s costs by half a percent net, that means the average
ACO is receiving about half of that tiny savings in the form of shared savings
payments, i.e., somewhere between zero and a quarter of a percent. And that in
turn means the average ACO is losing money. Our commonsense tells us that has
to be true because we know no human enterprise can operate without at least
some overhead costs, and the overhead costs incurred by ACOs have to be a lot higher
than one-fourth of a percent.
So, you ask, how high are Medicare ACO overhead costs?
Surely after 14 years and four ACO programs, CMS, the ACO industry, and health
services researchers have published research on this issue. Wrong. The only
information we have are occasional statements by MedPAC, based on nothing more
than a few interviews with ACO managers, that ACO administrative costs total
approximately 2 percent. MedPAC informs us, moreover, that this number does not
include extra services given to patients by ACOs in their (largely futile)
efforts to cut net Medicare spending. Those two numbers together –
administrative costs plus the cost of additional services delivered directly to
patients such as educational and transportation services – may well exceed ten
percent of total Medicare Part A and B spending attributable to some or most
ACOs. [3]
Even
if ACO overhead is just 2 percent, what possible rationale is there for
continuing the ACO experiment, much less for forcing doctors to choose between
joining an ACO and giving up their FFS Medicare practice? There is none.
Learning from the crash of lead
balloons
How
do we explain MedPAC’s obtuse behavior?
Unfortunately, this problem is not peculiar to MedPAC, it’s just more visible within MedPAC because, unlike the numerous other institutions that endorse evidence-free health policy, the commission’s deliberations are public. MedPAC’s dysfunctional thinking reflects habits of thought generated within the larger culture created by the managed care movement decades ago (for a longer discussion of this culture, see pp. 154-170 of my article with Ted Marmor). These habits of thought – a preference for abstraction, frequent use of labels designed to manipulate rather than inform (i.e. “accountable care”), and a cavalier attitude toward evidence (i.e., no interest in ACO overhead costs and misrepresentation of research on ACOs) – are rarely challenged by MedPAC members, in part because experts who don’t exhibit these habits of thought are rarely appointed to the commission. And on the infrequent occasion when those habits are challenged by one of the commissioners, no discussion ensues.
The
commission’s failure to discuss Jon Christianson’s unvarnished criticism of
ACOs at its April 4 meeting is a good example. In addition to asserting that
ACOs are not saving money, he warned his fellow commissioners that ACOs are even
less likely to work today than five years ago because of the rapid
consolidation of the system. He cited the recent “Aetna-CVS kind of vertical
merger, [and] all of the horizontal mergers that we’ve seen in the hospital industry.”(p. 76) The response? Crickets.
Because
MedPAC has been such a prolific endorser of evidence-free health policy fads (pay-for-performance
[P4P], incentives to buy electronic medical records, “medical homes,” ACOs,
punishment for “excess readmissions,” etc.), it is conceivable the commission’s
devotion to orthodoxy will eventually be undermined by reality – by a string of
undeniable failures of programs MedPAC recommended. MedPAC’s endorsement of P4P
in the early 2000s and its subsequent retraction of P4P for individual doctors
(as opposed to groups) illustrates this possibility. In 2015, Congress accepted
the advice of MedPAC and other managed care proponents and enacted what may be
the planet’s largest P4P program – the doomed Merit-based Incentive Payment
System (MIPS) (it was part of the MACRA law). At that point, MedPAC resembled
the dog that caught the car. They had what they had been recommending for over
a decade, and now it didn’t look like anything they could use. After a long
delay, MedPAC voted (on January 11, 2018) to urge Congress to repeal MIPS.
Was
the MIPS vote an aberration? Let us hope not.
Kip Sullivan is a member of the Health Care for All Minnesota advisory board and of the Minnesota chapter of Physicians for a National Health Program.
Footnotes
[1]
The table does not list two smaller ACO
programs run by CMS – a demonstration for dialysis centers, and a one-ACO
program for Vermont known as the Vermont All-Payer ACO Model demonstration.
[2]
In this footnote I’ll introduce the reader to the main issues raised by those ACO
proponents who argue that CMS’s use of historical controls is not as accurate
as research using concurrent controls. I’ll begin by noting, as I did in the
text, that this argument can’t explain the paltry three-tenths-of-a-percent
savings for the PGP demonstration. CMS used a concurrent control group in that
demo.
For
the three post-2012 programs (Pioneer, MSSP, and Next Generation), CMS has used
historical control groups against which to measure ACO success or failure. CMS constructs
these control groups first by assigning Medicare beneficiaries to ACOs based on
which primary care doctors Medicare beneficiaries saw during a three-year
look-period, that is, the three years preceding the performance year. CMS then calculates
the expenditures on these assignees during the look-back period and, after
making several adjustments including building in an increase to reflect
inflation during the performance year, sets a target for the performance year. Thus,
the assignees during the three-year look-back period serve as the controls for
the performance year.
The
critics of CMS’s method allege that CMS’s historical controls don’t adjust ACO
performance to take account of confounding factors as well as concurrent
control groups would. Why this should be so is never explained clearly. Both
forms of controls have advantages and disadvantages. The estimates derived with
the use of concurrent controls may be inferior because the construction of
concurrent controls introduces serious confounding factors which are not
introduced by historical controls and which are difficult to measure accurately.
The most serious of these is the necessity of changing the pool of
beneficiaries who were in the ACOs during the time period studied. McWilliams,
for example, altered the real-world pool of ACO assignees (the experimental
group) by making up his own assignment algorithm – an algorithm that differs
substantially from the one CMS uses.
A
second serious defect in concurrent-control studies is their use of CMS’s real-world
shared savings payments to ACOs to calculate the net savings or losses. What is
the logic of calculating gross savings or losses using a pool of assignees that
was different from the real-world pool, and then using only the real-world data
on CMS payments to ACOs to calculate the net?
[3]
The 2 percent figure for ACO overhead (the percent of Part A and Part B
spending attributed to an ACO that is eaten up by the cost of administering the
ACO) has appeared in at least two MedPAC documents – the transcript of the September 11, 2014 MedPAC meeting, and
MedPAC’s June 2018 report to Congress.
According to the transcript of the September 2014 meeting, then-commissioner David Nerenz asked MedPAC staffer Jeff Stensland if “we know anything about” ACO “overhead.” Stensland replied, “[P]eople we talk to and the data we have seen, it looks like maybe 1 to 2 percent of your spend, that that’s what they’re spending on their ACO to operate it….” (p 133). Stensland concluded, “[I]f you averaged everybody [that is, all ACOs] … the share of savings … that they get is going to be less than their administrative costs….” (p. 144)
MedPAC’s June 2018 report to Congress stated: “Our discussions with ACOs suggest their administrative costs, in contrast to those of MA plans, are close to $200 per beneficiary per year,” or about 2 percent of the $10,000 it costs Medicare to cover Part A and Part B expenses.
But
judging from the way the June 2018 report described “administrative costs,”
that 2 percent estimate is way below total ACO overhead – administrative costs
plus the costs ACOs incur to finance the interventions they hope will reduce
Medicare spending. Here’s how the June 2018 report described administrative
costs: “ACOs do not have the costs of advertising, enrolling, negotiating
contracts, and paying claims. Their administrative costs include the expense of
setting up and managing the ACO, which should include data analysis and
reporting quality measures.” (p. 236) That definition obviously excludes other
ACO-related costs, notably the cost of services delivered directly to patients that
are supposed to reduce billable Medicare services. These additional services
require hiring new staff, such as nurses and social workers and cab drivers, or
changing the job descriptions of existing staff.
What might those additional services cost? Again, we have almost no information. We get some idea of how extensive, and expensive, these services can be by examining a list of such services provided by Partners Healthcare Systems’ ACO (the second-largest of the 32 original Pioneer ACOs) to 4,000 of its sicker assignees. I extracted the list below from RTI International’s 2010 evaluation of Partners’ “care management program” (CMP). According to a 2017 report by John Hsu et al., that program constituted most of the interventions Partners’ ACO financed in its futile attempt to save money for Medicare. Here is the list:
“Eleven nurse case
managers [each of whom worked with about 200 patients] who received guidance
from the program leadership and support from the project manager, an
administrative assistant, and a community resources specialist” (p. 7);
“a social worker to
assess the mental health needs of CMP participants” (p. 6);
“a mental health team
director, clinical social worker, two psychiatric social workers, and a
forensic clinical specialist (M.D./J.D.), who follows highly complex patients
with issues such as legal issues, guardianship and substance abuse” (p. 10);
“a pharmacist to
review the appropriateness of medication regimens” (p. 6);
“home delivery of
medications five days per week” (p. 7);
“a nurse who
specialized in end-of-life-care issues” (p. 7);
“a patient financial
counselor who provided support for all insurance related issues” (p. 7);
“The clinical team
leader provided oversight and supervision of case managers” (p. 8);
“The medical director provided
oversight and day to day management of MGH’s [Massachusetts General Hospital’s]
CMP….” (p. 8);
“MGH developed a
series of clinical dashboards using data from the MGH electronic medical record
…, claims data, and its enrollment tracking database” (p. 8);
“MGH provided [200]
physicians with a $150 financial incentive per patient per year to help cover
the cost of physician time for [CMP-related] activities” (p. 8);
“a designated case
manager position to work specifically on post discharge assessments to enhance
transitional care monitoring” (p. 9);”
“a data analytics team to develop and strengthen
program’s reporting capabilities” (p. 10); and
numerous housing,
transportation and other “support services” and “community services” (p. 6) that
RTI described only vaguely.