Joining Matthew Holt (@boltyboy) on #THCBGang on Thursday August 31 at 1pm PST 4pm EST are the small but mighty pairing of Kim Bellard (@kimbbellard); and patient safety expert and all around wit Michael Millenson (@mlmillenson).
You can see the video below & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.
Editor Note: This article was published a week after the Republican Party Primary debate
BY MIKE MAGEE
This evening, the Republican Party will sponsor their first Primary Debate. It will be historic in featuring the absence of their lead contender for the 2024 Presidential campaign, a candidate who appears committed to the destruction of their own political party
Events over the past year clearly have confirmed that we are a “work in progress” even as we stubbornly affirm our good intentions to create a society committed to “life, liberty, and the pursuit of happiness.”
With the Dobbs’ decision, our Supreme Court has unleashed long-abandoned regressive state laws designed to reinforce selective patriarchy and undermine the stability and confidence of America’s women and families. As a result, our nation’s health professionals, and the patients they care for, potentially find themselves “on the wrong side of the law.”
Three months ago, our former President decided to deliver a message to North Carolina Republican supporters claiming that he was engaged in the “final battle” with “corrupt” forces, most especially the “Deep State” that was “out to get him.” This is the same state that politically birthed Mark Meadows, former Congressman from the 11th District of North Carolina, a position he resigned to become Trump’s Chief of Staff on March 21, 2020. That ultimately landed him a position on the roster of 19 individuals indicted by District Attorney Fani Willis on RICO charges for conspiracy and racketeering.
Trump and Meadow’s actions stand in stark contrast to the ethics and values I experienced in the UNC surgery program in Chapel Hill, NC, from 1973 to 1978. They also do not reflect the standards advanced in North Carolina’s K-12 lesson plan, titled “The Rule of Law,” which begins with the Teddy Roosevelt quote, “No man is above the law, and no man is below it” from his 1903 State of the Union address.
The plan affirms that law is fundamental to societal health stating:
“The rule of law is basically an agreement that everyone will play by the rules. This allows us to enjoy a more peaceful and safe existence. The rule of law also ensures the protection of certain rights for each of us. Ideally, the rule of law applies equally to everyone, meaning you are treated fairly and equally, under the same set of rules, regardless of who you are.”
The curricular plan asks a question I’d love to hear FOX news co-moderators Bret Baier and Martha MacCallum, ask this evening.
“How do laws affect each of us, and what functions do laws serve in our society?
According to the NC curricular plan, here are the answers the K-12 teachers (and tonight’s FOX moderators) should be looking for.
1.“Laws serve as standards of conduct…
2. Laws maintain order, ensure predictability, and provide security.
3. Many laws in America grant and protect particular individual rights and freedoms, ensure equality, and advocate for the common good.
4. Laws guarantee certain benefits to citizens (e.g., schools, health services, etc.)
5. Laws assign responsibilities to citizens (e.g., paying taxes.)
6. Laws define what duties the government will perform and can also limit the power of governmental officials.
7. Laws can facilitate different forms of change (e.g., toxic waste disposal, anti-discrimination, prohibition of spousal abuse, etc.)
8. Laws are used to manage different forms of conflict, relying on courts, lawyers, and judges for such.
9. Ideally, laws should be well designed to ensure justice; they should be designed so that the average citizen can interpret, understand, and thus follow them.”
When I first read the reports about some Silicon Valley billionaires wanting to start a new city, I figured, oh, it’s just a bunch of rich white guys wanting to take their toys and go to a new, better home. After all, they’ve seen what’s been happening to downtown San Francisco (or Portland, or Chicago – pick your preferred city).
Cities these days may be an what one expert calls an “urban doom loop” – struggling to recover after having been hollowed out by the pandemic. These so-called elites probably figured it’s easier to build something new rather than to try to fix what already exists. And, you know, they may be right.
Now that I think about it, the same may be true of our healthcare system.
The group, fronted by a mysterious entity called Flannery Associates, has been busy buying up land outside San Francisco for the past five years, spending a reported $1b for some 57,000 acres in Solano County. The proximity of its purchases to Travis Air Force Base had already raised concerns. Believed to be behind the group are a number of well known tech names, including LinkedIn co-founder Reid Hoffman; former Sequoia Capital partner Michael Moritz; venture capitalists Marc Andreessen and Chris Dixon; Stripe co-founders Patrick Collison and John Collison; Laurene Powell Jobs, Steve Jobs widow.
It doesn’t help that earlier this year Flannery sued dozens of local landowners for colluding to drive up prices, or that they’ve been so secretive. John Garamendi, one of the area’s Congressmen, said: “Flannery Associates has developed a very bad reputation in Solano County through their total secrecy and mistreatment of generational family farmers.”
The group finally went public with its intentions last week. “We are proud to partner on a project that aims to deliver good-paying jobs, affordable housing, clean energy, sustainable infrastructure, open space and a healthy environment to residents of Solano County,” said spokesman Brian Brokaw. “We are excited to start working with residents and elected officials, as well as with Travis Air Force Base, on making that happen.”
Most of the land is currently zoned for agricultural use, so getting permission for residential or other business uses will take some effort, which is why Flannery Associates is planning to meet with local, state, and federal officials.
The New York Timesreported that Mr. Moritz spearheaded the effort in 2017, sending out a note: “He painted a kind of urban blank slate where everything from design to construction methods and new forms of governance could be rethought.” A poll sent out last week to Solano County residents asked if they’d be in favor of a ballot initiative that would “include a new city with tens of thousands of new homes, a large solar energy farm, orchards with over a million new trees, and over 10,000 acres of new parks and open space.”
What’s not to like?
If this is going to be another enclave of rich people,then I hope it never gets off the ground, after burning off lots of their money (not that they’d miss it). If they’re sincere about having a diverse city, all incomes and racial/ethnic backgrounds, then I’ll be watching closely. They have a chance to build new infrastructure (hint: include robust wastewater monitoring!), ensure safe and affordable housing for all, use renewable energy, design it for walkability, and fill it with plenty of green space. They could hire the good people at Building H to help “build health into everyday life.” And if they really want to impress me, they could even replicate/expand on Stockton’s universal basic income initiative.
But what are they going to do about health care? What’s the point of building a 21st century city from scratch only to overlay it with our 20th century healthcare system — the notoriously frugal Medi-Cal program, scads of employer health plans, and ACA individual plans, not to mention Medicare/Medicare Advantage for any seniors who happen to end up there. There’ll be lots of hospitals and specialists who might see the new city as a great chance to make lots of money from all those private pay patients. It will be our familiar mess.
No, if they want to do this right, they should rethink health care too. Here’s a few ideas they should consider:
Universal coverage: if you live in the community, you’re covered. No exceptions, no opt-outs, no ineligibles. Think of it as their own group health plan. They might need some Medicaid and Medicare waivers to do this right, but they should make this the first community where everyone is covered.
Wealth-based funding: everyone should participate in how the healthcare system is funded, but not through the inequitable premium system we’re used to but through taxes on income, wealth, and/or property. No one should ever be priced out of coverage (or care).
Health, not medical: we always say “healthcare system” but what we mean is our medical care system. It’s built around doctors, hospitals, and other medical professionals and institutions. They’re all part of it, but they’ve become the tail that wags the dog. Nutrition, exercise, sleep, social support, and so many other factors contribute far more to our health. These shouldn’t be ancillary to the new system but integral to it, with medical care what happens only when those don’t suffice.
Primary care emphasis: the system should focus on recruiting (and retaining) enough primary care physicians (including OB/GYNs and mental health professionals) that waits are nominal, visits aren’t rushed, and primary care is the main locus of care. Forget traditional fee schedules/salaries; make income for primary care commensurate with its value.
Tech enabled: the Silicon Valley folks should love this: the system should be designed around the latest tech – e.g., virtual care. real-time monitoring (e.g., wearables), AI support, and so on, along with proactive Big Data analysis and recommendations. And do better than Epic!
Hospitals: to be honest, I’m not sure there should be any hospitals, at least not initially. Don’t build any big buildings that become capital sinks. Maybe let the Johns Hopkins (or other) experts design a Hospital At Home program that suits the community, keeping people in their homes. Only build physical hospital(s) when the population warrants it, and even then build them as small as possible. And certainly don’t let them employ physicians.
That’s not an all-encompassing list, but it’s a start.
————–
I’m not holding my breath that Flannery Associates will build their new utopia, but, let’s admit it, they have a better chance than they do to create a 21st-century healthcare system.
Kim is a former emarketing exec at a major Blues plan, editor of the late & lamented Tincture.io, and now regular THCB contributor.
This is the last of the classics that THCB will run to celebrate our 20th birthday. And we are finally tackling the most important of questions. Is what we call this thing one word or two? Back in 2012 Michael Millenson had the definitive answer–Matthew Holt
By MICHAEL L. MILLENSON
A recent contributor to this blog wondered about the correctness of “health care” versus “healthcare.” I’d like to answer that question by channeling my inner William Safire (the late, great New York Times language maven). If you’ll stick with me, I’ll also disclose why the Centers for Medicare & Medicaid Services is not abbreviated as CMMS and reveal something you may not have known about God – linguistically, if not theologically.
The two-word rule for “health care” is followed by major news organizations (New York Times, Washington Post, Wall Street Journal) and medical journals (New England Journal of Medicine, JAMA, Annals of Internal Medicine). Their decision seems consistent with the way most references to the word “care” are handled.
Even the editorial writers of Modern Healthcare magazine do not inveigh against errors in medical care driving up costs in acutecare hospitals and nursinghomes. They write about “medical care,” “acute care” and “nursing homes,” separating the adjectives from the nouns they modify. Some in the general media go even farther, applying the traditional rule of hyphenating adjectival phrases; hence, “health-care reform,” just as you’d write “general-interest magazine” or “old-fashioned editor.”
Most importantly of all, the Associated Press decrees that the correct usage is, “health care.” That decision is not substantive – there is absolutely no definitional difference between “health care” and “healthcare,” despite what you might read elsewhere — but stylistic. As in The Associated Press Stylebook.
The AP is a cooperative formed back in 1846 by newspapers to share reporting via a wire service. Today, the AP calls itself the backbone of global news information, serving “thousands of daily newspaper, radio, television, and online customers….On any given day, more than half the world’s population sees news from the AP.” When that news arrives in text format, its spelling is determined by the AP stylebook. Which means a few billion people see the spelling, “health care.”
A stylebook? Isn’t spelling determined by dictionaries? Perhaps, but when you’re sharing content on deadline across the world, it helps if everyone agrees to refer to, say, the Midwest, not the Mid-West, and to use other common linguistic conventions.
Stylebooks differ. The AP would say that health care is two words; the Chicago Manual of Style, popular in academia, would write that as 2 words, but agree with the premise.
So why isn’t that the end of the issue? Because conventions are not set in concrete. For example, at the time the Internet first became popular, the AP preferred the term “Web site” over “website” because the World Wide Web is a proper name. A successful lobbying campaign on behalf of the lower-case form helped persuade the AP to adopt the new spelling in its 2010 stylebook update.
When Modern Hospitals changed its name to become Modern Healthcare back in 1976, it did so in part to seem, well, modern. It hadn’t been that many years, after all, since airplanes were flown by air lines, not airlines. Then, in the business-oriented 1980s, “healthcare system” became a convenient linguistic upgrade of the dowdy “hospital” that had gobbled up ownership of doctors’ offices providing outpatient (not out-patient) care.
At the same time, a growing number of companies decided to make this expansive new word part of their proper name or, at the very least, their style sheet. For instance, HCA, founded in 1968 as Hospital Corporation of America, today describes itself as “the nation’s leading provider of healthcare services.” The Reuters news service, heavily involved in business news, now uses “healthcare” in its stories.
The 2001 Institute of Medicine report Crossing the Quality Chasm provides a snapshot of the term’s transition. The report declares, “Between the healthcare we have and the care we could have lies not just a gap, but a chasm.” The author of that ringing statement is the Committee on the Quality of Health Care in America.
However, I think a tipping point for fusing “health” and “care” was reached with the federal legislation setting up the Agency for Healthcare Research and Quality at the end of 1999. AHRQ was a renamed and refocused version of the old Agency for Health Care Policy and Research, created in 1989. AHCPR, in turn, had almost been named the Agency for Health Care Research and Policy until an alert Senate staffer realized that the abbreviation would be pronounced, “ah, crap.”
Speaking of abbreviations, Tom Scully, the first administrator of the Center for Medicare & Medicaid Services, once explained to me why it is known as CMS, not CMMS. It seems that Health and Human Services Secretary Tommy Thompson wanted an agency name with a catchy three-letter abbreviation, like FTC or CIA, to replace the old HCFA (Health Care Financing Administration). So a legal opinion was obtained from the HHS counsel that employing an ampersand to separate the words “Medicare” and “Medicaid” permitted the use of the CMS designation. Some might suspect this Solomonic ruling of caving in to a bit of pressure from above.
Which brings us to God. Some years back, the AP decided that while “God” would remain capitalized (the pope was not similarly blessed), the second reference would be “his,” not “His.” As influential as the AP might be in this world, those concerned with a Higher Authority still write about God as if He were something more than an ordinary man.
I keep waiting for the AP editor who made that decision to be struck down with lightning by the Deity. But, on the other hand, She may have a sense of humor.
Michael Millenson is a Highland Park, IL-based consultant, a visiting scholar at the Kellogg School of Management and the author of “Demanding Medical Excellence: Doctors and Accountability in the Information Age”.
As the 20th Birthday rolls on I thought I’d bring out a more recent piece first published in October 2020, albeit one that relies heavily on 25 year old data to make a point. This is some evidence to back up Jeff Goldsmith’s comment on the original that for all the talk “ ‘Value based” payment is a religious movement, not a business trend’ ” By the way, Humana updated these numbers last year and there’s been basically no change — Matthew Holt
By MATTHEW HOLT
Humana is out with a report saying that its Medicare Advantage members who are covered by value-based care (VBC) arrangements do better and cost less than either their Medicare Advantage members who aren’t or people in regular Medicare FFS. To us wonks this is motherhood, apple pie, etc, particularly as proportionately Humana is the insurer that relies the most on Medicare Advantage for its business and has one of the larger publicity machines behind its innovation group. Not to mention Humana has decent slugs of ownership of at-home doctors group Heal and the now publicly-traded capitated medical group Oak Street Health.
Humana has 4m Medicare advantage members with ~2/3rds of those in value-based care arrangements. The report has lots of data about how Humana makes everything better for those Medicare Advantage members and how VBC shows slightly better outcomes at a lower cost. But that wasn’t really what caught my eye. What did was their chart about how they pay their physicians/medical group
What it says on the surface is that of their Medicare Advantage members, 67% are in VBC arrangements. But that covers a wide range of different payment schemes. The 67% VBC schemes include:
Global capitation for everything 19%
Global cap for everything but not drugs 5%
FFS + care coordination payment + some shared savings 7%
FFS + some share savings 36%
FFS + some bonus 19%
FFS only 14%
What Humana doesn’t say is how much risk the middle group is at. Those are the 7% of PCP groups being paid “FFS + care coordination payment + some shared savings” and the 36% getting “FFS + some share savings.” My guess is not much. So they could have been put in the non-VBC group. But the interesting thing is the results.
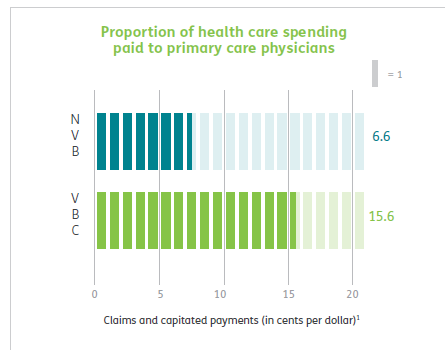
First up Humana is spending a lot more on primary care for all their VBC providers, 15% of all health care spend vs 6.6% for the FFS group, which is more than double. This is more health policy wonkdom motherhood/apple pie, etc and probably represents a lot of those trips by Oak Street Health coaches to seniors houses fixing their sinks and loose carpets. (A story often told by the Friendly Hills folk in 1994 too).
But then you get into some fuzzy math.
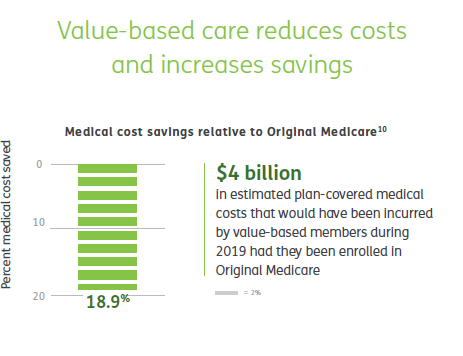
According to Humana their VBC Medicare Advantage members cost 19% less than if they had been in traditional FFS Medicare, and therefore those savings across their 2.4m members in VBC are $4 billion. Well, Brits of a certain age like me are wont to misquote Mandy Rice-Davis — “they would say that wouldn’t they”.
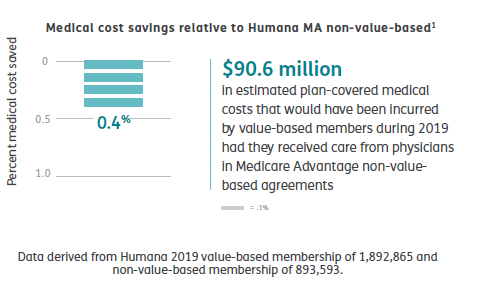
But on the very same page Humana compares the cost of their VBC Medicare Advantage members to those 33% of their Medicare Advantage members in non-VBC arrangements. Ponder this chart a tad.
Yup, that’s right. Despite the strung and dram and excitement about VBC, the cost difference between Humana’s VBC program and its non-VBC program is a rounding error of 0.4%. The $90m saved probably barely covered what they spent on the fancy website & report they wrote about it
Maybe there’s something going on in Humana’s overall approach that means that FFS PCPs in Medicare Advantage practice lower cost medicine that PCPs in regular ol’ Medicare. This might be that some of the prevention, care coordination or utilization review done by the plan has a big impact.
Or it might be that the 19% savings versus regular old Medicare is illusionary.
It’s also a little frustrating that they didn’t break out the difference between the full risk groups and the VBC “lite” who are getting FFS but also some shared savings and/or care coordination payments, but you have to assume there’s a limited difference between them if all VBC is only 0.4% cheaper than non-VBC. Presumably, if the full risk groups were way different they would have broken that data out. Hopefully they may release some of the underlying data, but I’m not holding my breath.
Finally, it’s worth remembering how many people are in these arrangements. In 2019 34% of Medicare recipients were in Medicare Advantage. Humana has been one of the most aggressive in its use of value-based care so it’s fair to assume that my estimates here are probably at the top end of how Medicare Advantage patients get paid for. So we are talking maybe 67% of 34% of all Medicare recipients in VBC, and only 25% of that 34% = 8.5% in what looks like full risk (including those not at risk for the drugs). This doesn’t count ACOs which Dan O’Neill points out are about another 11m people or about 25% of those not in Medicare Advantage. (Although as far as I can tell Medicare ACOs don’t save bupkiss unless they are run by Aledade).
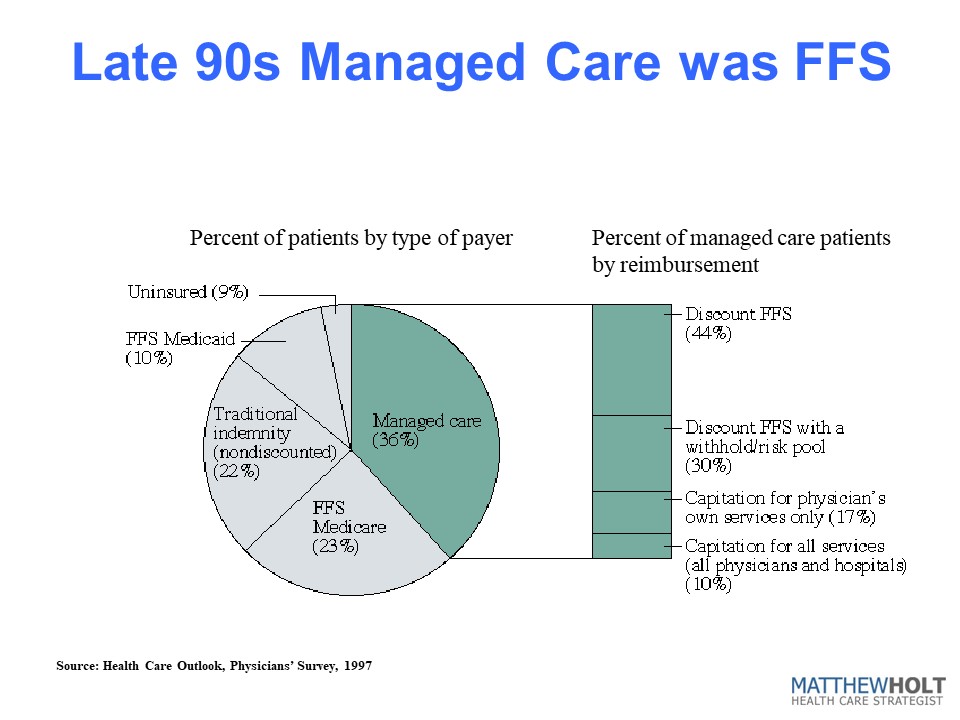
I did a survey in 1997 which some may recall as the height of the (fake) managed care revolution. Those around at the time may recall that managed care was how the health insurance industry was going to save America after they killed the Clinton plan. (Ian Morrison used to call this “The market is working but managed care sucks”). At the time there was still a lot of excitement about medical groups taking full risk capitation from health plans and then like now there was a raft of newly publicly-traded medical groups that were going to accept full risk capitation, put hospitals and over-priced specialists out of business, and do it all for 30% less. The Advisory Board, bless their very expensive hearts, put out a report called The Grand Alliance which said that 95% of America would soon be under capitation. Yeah, right. Every hospital in America bought their reports for $50k a year and made David Bradley a billionaire while they spent millions on medical groups that they then sold off at a massive loss in the early 2000s. (A process they then reversed in the 2010s but with the clear desire not to accept capitation but to lock up referrals, but I digress!).
In the 1997 IFTF/Harris Health Care Outlook survey I asked doctors how they/their organization got paid. And the answer was that they were at full risk/capitation for ~3.6% of their patients. Bear in mind this is everyone, not just Medicare, so it’s not apples to apples with the Humana data. But if you look at the rest of the 36% of their patients that were “managed care” it kind of compares to the VBC break down from Humana. There’s a lot of “withholds” which was 1990s speak for shared savings and discounted fee-for-service. The other 65% of Americans were in some level of PPO-based or straight Medicare fee-for-service. Last year I heard BCBS Arizona CEO Pam Kehaly say that despite all the big talk, the industry was at about 10% VBC and the Humana data suggests this is still about right.
So this policy wonk is a bit depressed, and he’s not alone. There’s a little school of rebels (for example Kip Sullivan on THCB last year) saying that Medicare Advantage, capitated primary care and ACOs don’t really move the needle on cost and anyway no one’s really adopted them. On this evidence they’re right.
Matthew Holt is the Publisher of THCB and is still allowed to write for it occasionally.
Since the early days of the pandemic, conspiracy theorists have charged that COVID was a manufactured bioweapon, either deliberately leaked or the result of an inadvertent lab leak. There’s been no evidence to support these speculations, but, alas, that is not to say that such bioweapons aren’t truly an existential threat. And artificial intelligence (AI) may make the threat even worse.
Last week the Department of Defense issued its first ever Biodefense Posture Review. It “recognizes that expanding biological threats, enabled by advances in life sciences and biotechnology, are among the many growing threats to national security that the U.S. military must address. It goes on to note: “it is a vital interest of the United States to manage the risk of biological incidents, whether naturally occurring, accidental, or deliberate.”
“We face an unprecedented number of complex biological threats,” said Deborah Rosenblum, Assistant Secretary of Defense for Nuclear, Chemical, and Biological Defense Programs. “This review outlines significant reforms and lays the foundation for a resilient total force that deters the use of bioweapons, rapidly responds to natural outbreaks, and minimizes the global risk of laboratory accidents.”
And you were worried we had to depend on the CDC and the NIH, especially now that Dr. Fauci is gone. Never fear: the DoD is on the case.
A key recommendation is establishment of – big surprise – a new coordinating body, the Biodefense Council. “The Biodefense Posture Review and the Biodefense Council will further enable the Department to deter biological weapons threats and, if needed, to operate in contaminated environments,” said John Plumb, Assistant Secretary of Defense for Space Policy. He adds, “As biological threats become more common and more consequential, the BPR’s reforms will advance our efforts not only to support the Joint Force, but also to strengthen collaboration with allies and partners.”
Which is scarier: that DoD is planning to operate in “contaminated environments,” or that it expects these threats will become “more common and more consequential.” Welcome to the 21st century.
The report specifically calls out Iran, North Korea, the People’s Republic of China (PRC), and Russia as having the knowledge and capabilities for such weapons, and assesses that North Korea and Russia still possess offensive biological weapons (it suspects Iram does too, and notes that China considers biology “a new domain of war”). China and Russia “have also proven adept at manipulating the information space to inhibit attribution, to reduce trust and confidence in countermeasure effectiveness, and potentially to slow decision-making following deliberate use.”
It directs further attention to China: “The United States has compliance concerns with respect to PRC military medical institutions’ toxin research and development given their potential as a biothreat. The PRC has also released plans to make China the global leader in technologies like genetic engineering, precision medicine, and brain sciences.”
Asha M. George, executive director at the Bipartisan Commission on Biodefense, told The Washington Post. “I would not be surprised if by next year they’re saying China has some offensive biological weapons programs. Usually, they just say something like, you are concerned about dual use. And this year they didn’t do that,” He added that Russia remains an equally concerning threat.
Here’s where it gets really scary:
New technologies, such as big data, artificial intelligence, and genomic modification, have the potential to significantly influence the chemical, biological, radiological, and nuclear (CBRN) environment. Such technologies simultaneously offer the prospect for more effective, resilient, and cost-efficient military and civilian solutions while also representing potential new threats from state and non-state actors. The same biological and chemical science advancements created to develop life-saving medical countermeasures could also be used by potential adversaries to develop new or enhanced agents. Technologies intended to reduce testing and production inefficiencies, such as biofoundaries and additive manufacturing, create opportunities to reduce the development footprint and increase the number of proliferation pathways available to malign actors. In this way, emerging and disruptive technologies present both risks and opportunities to the United States, its allies, and partners.
Writing in Vox, Jonas Sandbrink, a biosecurity researcher at the University of Oxford, similarly warns: “large language models (LLMs) like ChatGPT, as well as novel AI-powered biological design tools, may significantly increase the risks from biological weapons and bioterrorism.” AI-powered biological design tools (BDTs), he says, “could allow the design of biological agents with unprecedented properties.” E.g., ones without any evolutionary constraints or precedents.
Obviously, we need more and better oversight over not just bioweapons but also AI generally, but the fear is that bad actors – whether nations or malign individuals/groups – probably won’t feel constrained by any rules or guidelines such oversight degrees. Even U.S. Senators, not known for their technical prowess, expressed alarm in a recent hearing.
One witness at the hearing, Dario Amodei, chief executive of the AI company Anthropic, warned: “certain steps in bioweapons production involve knowledge that can’t be found on Google or in textbooks and requires a high level of expertise. We found that today’s AI tools can fill in some of these steps.” He thinks an AI-bioweapon is a “medium-term risk,” and by that he meant: “Whatever we do, it has to happen fast…I would really target 2025, 2026, maybe even some chance of 2024.”
The only thing that has remotely offered me any hope is that, whatever DoD or others are doing, DARPA is already working on it. It established its Biological Technologies Office (BTO) in 2014, recognizing “the vanishing of once longstanding gaps between the life sciences, engineering, and computing disciplines.” One of the key capabilities DARPA is focusing on “is creating innovative biotechnological approaches to rapidly detect and characterize these threats, preventing surprise and maintaining force readiness.”
Sure, DARPA is focused on the military, but if its work on the Internet and GPS, among others, ended up with wide-reaching civilian applications, one would hope that its efforts here would as well. There’s no point to the military surviving a bioweapon attack if all the civilians end up dead.
—————
With synthetic biology, gene editing, and other biological tools, creating bioweapons is or will soon become much easier, and perhaps much more powerful, than building nuclear weapons. With AI, that will happen much quicker and perhaps become even more dangerous.
The genie is not going back in the box. We’re not going to unlearn all we now know about manipulating biology. We’re not going to stop using AI. Like all tools, though, they’re neither good nor evil; only how we use them is. Let’s hope we use these right.
Kim is a former emarketing exec at a major Blues plan, editor of the late & lamented Tincture.io, and now regular THCB contributor.
Early this month I caught up with Torben Nielsen who is now CEO of Uptiv Health. Another one from the Redesign Health factory, Uptiv Healthcame out of stealth recently with the goal of improving the experience and reducing the cost of those patients who have to have regular infusion treatments. Uptiv Health just raised $7.5m and is opening its first location in Detroit at the end of August 2023, with a goal of becoming the health home of those chronic disease patients. Why do we need a new offering in infusion care? Torben will tell you–Matthew Holt
On September 25, 1939, Southern California woke with fear of The Lash of St. Francis or El Cordonazo on the horizon. The term refers to northwestern tracking, cyclone-laden storms that can hit the western shores of Mexico and California most commonly around the Feast of Saint Francis, on October 4th. This one made landfall at San Pedro, California.
The calamity that day in Southern California was a rare event, the only one of its kind in the 20th century. The last one to hit, prior to this was in San Diego on October 2,1858. The Earth’s rotation normally assures that such cyclones in this region move from east to west, and out to sea. But the 1939 storm was the exception, and the big problem was the rain, some 5 1/2 inches over a 24-hour period (though the town of Indio, in the Coachella Valley of Southern California’s Colorado Desert region experienced 7 inches and buried the valley in 4 feet of water. Forty-five died on land, and 48 perished at sea. One positive – the storm marked the end of a 1-week heat wave where Los Angeles reached 107 F degrees and claimed 100 lives.
History repeated itself 84 years later this weekend, with a memorable “Lash” on the backend of a summer heat wave. The human, economic, and ecological tolls remain to be calculated. But one thing is for certain, global warming has arrived, and with it the production of both heat and water and a new, all too familiar meteorological phenomenon, the “atmospheric river.”
NOAA defines “atmospheric river” this way: “Atmospheric rivers are relatively long, narrow regions in the atmosphere – like rivers in the sky – that transport most of the water vapor outside of the tropics. While atmospheric rivers can vary greatly in size and strength, the average atmospheric river carries an amount of water vapor roughly equivalent to the average flow of water at the mouth of the Mississippi River. Exceptionally strong atmospheric rivers can transport up to 15 times that amount. When the atmospheric rivers make landfall, they often release this water vapor in the form of rain or snow.”
To be clear, these drenching above-ground collections of water are generally a blessing because they provide most of the much-needed precipitation to California’s dry areas and replenish the water cycles in the region. But as the Earth has warmed, they more frequently represent “too much of a good thing”, and are now responsible for 90% of California’s flood damage.
NASA reports that “the increases in water vapor are a consequence of global warming. Higher temperatures increase the evaporation of water over land and sea. The warmer area holds onto more water vapor, and slows down condensation and precipitation. The trapped water floating in the sky absorbs even more heat, which in turn attracts even more water vapor – creating a disastrous “positive feedback loop.”
By sucking up water vapor, the phenomenon makes dry regions drier, and by forming and dumping the “rivers”, creates wetter wet regions and tragic flooding. Specifically, here are five predictable repercussions of human behavior-induced alterations in global atmospheric health.
1. Heavier Rainfall: For every 1 degree Celsius (1.8 here F) rise in atmospheric temperature, the air is able to absorb 7% more water. Since the pre-industrial revolution, the atmospheric temperature has risen 1.3 degrees Celsius. By the end of this century, if trend lines are uninterrupted, rainfall amounts could increase up to 60% over current levels.
2. Massive Infrastructure Destruction: Flood damage in the billions is nearly certain as storms become more intense, prolonged, and closer spaced. Atmospheric river events could increase three or four-fold compared to pre-industrial times. Expect an additional $1 billion in flood damage for every 1 degree Celsius rise in temperature.
3. Diminished Snowpack Reserves: Atmospheric rivers are associated with less snowfall in western U.S. mountain ranges. Intense rainfall on existing snow accelerates melting and extreme flooding from rapid water runoff. Termed “rain-on-snow” events, areas at greatest risk are the Canadian Rockies, the Sierra Nevada, and the Colorado River network.
4. Geographic Shifts: Warmer atmospheres show signs of altering the jet stream, pushing it closer to the equator. Experts have predicted that this will result in the winter expansion of atmospheric river events in Southern California. Paradoxically, soils are drying out due to increased soil evaporation, less snowpack cover, and erosion from rapid downpours.
5. Loss of Sea Ice: Recent studies reveal that shrinking ice cover in the Artics is not simply a function of warming temperatures. A new contributor is that the atmospheric rivers are increasingly moving north toward the Arctic Pole. It is now believed that the resultant water on ice is responsible for at least 1/3 of the loss of winter ice. They do this not only by the melting effect of direct water on ice over 10 days following each downpour but also by magnifying “downward longwave radiation”
As this most recent weather calamity confirms, human-instigated extreme climate-driven events are now inescapable in the short term. This storm is currently dumping 3 to 6 inches across the region, with 10 inches in some locations coming close to overwhelming the deep LA water trenches. Equally evident is that our modern (and aging) infrastructure – including roads, spillways, bridges, dams, building codes, and rescue and safety operations – require a rapid redesign.
One of the greatest pleasures of running THCB has been to get to know and host the writings of some of my health policy heroes. This week I have already published work from Jeff Goldsmith, and Ian Morrison & Michael Millenson among others will be featured next week (as the party won’t quite stop). Perhaps one of the most amazing things was that the doyen of health economists, Uwe Reinhardt, offered to write some original pieces for THCB…prodded by former editor John Irvine. This is one of my favorites, riffing on a talk I heard him give in (I think) 1993 about how HCFA was like the Kremlin and how free market Reaganite Republicans had made it so. This piece is from Jan 2017 and Uwe sadly died that November.–Matthew Holt
Although, unlike most other nations, the U.S. has only two parties worth the name, their professed doctrines compared with their actions strikes me as more confusing than the well-known Slutsky Decomposition which, as everyone knows, can be derived simply from a straightforward application of Kramer’s rule to a matrix of second partial derivatives of a multivariable demand function.
The leaders of the drug industry, for example, probably are now breaking out the champagne in the soothing belief that their aggressive pricing policies for even old drugs are safe for at least the next eight years from the allegedly fearsome, regulation-prone, price-controlling Democrats. My advice to them is: Cool it! Follow me through a brief history of Republican health policy, to learn what Republicans will do to the health-care sector when it ticks them off.
Republicans like to tar Democrats over allegedly socialist policy instruments such as price controls, global budgets and deficit-financed government spending. Democrats usually roll over to take that abuse, almost like hanging onto their posteriors signs that says “Kick me.” I say “abuse,” because Republicans have never shied away from using the Democrats’ allegedly left-wing tactics when health care chews up their budgets or turns voters against them.
Think of the early 1970s. Like most other economies in the world, the U.S. economy then suffered very high inflation, led by health spending widely judged to be out of control. So Republican President Richard Nixon thought nothing of slapping price controls onto the entire U.S. economy, keeping them longest on the health care sector. (I cannot imagine Democrats ever having the guts to do that or, for that matter, to sojourn to China, there to pay court to Mao Tse Tung, the self-anointed Communist Emperor of the Middle Kingdom).
Think of the 1980s. Ticked off by the ever increasing grab for taxpayers’ money triggered by Medicare’s retrospective reimbursement of hospitals then in place, Republican President Ronald Reagan thought nothing of slapping onto that sector a set of centrally administered Medicare prices for the whole country. That new pricing scheme, based on the Diagnosis Related Groupings (DRGs), reminds one of nothing so much as Soviet style pricing, to cite the mournful, subsequent mea culpa of one of the former bureaucrats tasked with implementing that system between 1983 and 1986.
I recall making in the early 1990s a presentation to the Missouri Hospital Association, where I opened up with the following slide:
(I actually wore that uniform at the podium. I had been bought by my wife, in 1989, from a Russian at the Brandenburg Gate in Berlin, immediately after the fall of the Berlin Wall. The photo was taken in 1990 by our son Mark, at the tank museum of the Aberdeen Proving Grounds in Maryland, before a WWII Russian T-62 tank.)
Evidently enchanted by the price-controlling, cost-containment power of President Reagan’s Soviet pricing scheme for hospitals, President George Herbert Walker Bush imposed, in 1992, a similar scheme on physicians treating Medicare patients. Known as Medicare Fee Schedule (MFS), it was based on the Resource-Based Relative Value Scale (RBRVS), a pseudo-scientific design that seeks to base relative Medicare fees for particular services on their relative cost of production. A problem with that approach, of course, is that relative costs do not coincide with relative values. It would set the fees for, say, a hypothetical transurethral tonsillectomy as much higher than that of the traditional transoral one, simply because the transurethral approach is more time consuming.
Anticipating that physicians would game the new Medicare Fee Schedule by responding to lowered fees with commensurate increases in the volume of services recommended and delivered to patients, the Bush Sr. Administration coupled the new fee schedule with Volume Performance Standards (VPS), a fancy euphemism for nationwide global budgets, one for surgical and the other for non-surgical physician services delivered to Medicare patients. Democrats may dream of global budgets. Republicans do them. That anyone seriously thought a global budget for as large an entity as the entire U.S. could ever work – that it was productive to punish conservatively practicing physicians in Duluth, Minnesota for huge volume increases in Dade Country, Florida — is a testimony to the far reaches of the human mind.
Predictably disenchanted with the non-performance of the Volume Performance Standards, a Republican House in 1997 morphed it into Medicare’s Sustainable Growth Rate (SGR). The SGR became law. It was global budgeting still for the entire nation, but so stringent that Congress dared apply it in only one year, otherwise kicking it down the road unused, for eventual resolution.
That resolution came in 2015, with the so-called “Doc Fix,” the still controversial Medicare Access and CHIP Reauthorization Act (MACRA). That act was sponsored and introduced to the Republican House of Representatives by a Republican Congressman from Texas who is also a physician. It was promptly signed into law by President Obama, after it was passed with a bi-partisan vote in both chambers. The MACRA quite sensibly seeks to establish a direct link between Medicare payments to a physician and the quality of the services delivered by that physician. Alas, once packaged by the bureaucracy into concrete regulations for operation in the trenches, the resulting complexity of measuring quality in practice and even the validity of these operational metrics now predictably has physicians all over the country up in arms.
And so it goes, to plagiarize Kurt Vonnegut.
So it is prudent to wonder just what health policy will come down in the years ahead from the Republican Mount Olympus ruled by President Trump. Republican Presidents, members of Congress and Governors may like playing golf with the leaders of the health-care industry and share a Bourbon or two with them; but they don’t like it when that industry’s endless, energetic search for mammon chews up their budgets, and they do not hesitate to react to that fiscal hemorrhaging with fury, often resorting to the allegedly socialist tactics they usually ascribe to the Democrats.
What can be said about health policy also applies to U.S. fiscal policy. Democrats have never been able to shake off the label that they are the party of deficit-financed government spending – that they practice the much maligned, socialist Keynesian economics — in spite of plenty of history to the contrary. Consider, for example, the graph below published by the non-partisan Congressional Budget office (CBO).
The time paths of federal tax revenues and spending clearly show what former Vice President Dick Cheney reportedly explained to an amazed then Secretary of the Treasury Paul O’Neill: “Reagan taught us that deficits don’t matter.”
Deficit financed government spending and tax cuts are usually considered the very core of Keynesian economics, aimed at shoring up the demand side of the economy. It is based on the idea that there is not enough demand to buy the products the supply side could deliver. It is a policy much decried by Republicans and the media supporting them, e.g., The Wall Street Journal or the anchors and talking heads on Fox News TV. It stands in contrast to so-called supply side economics, which seeks to rev up the economy by changing the financial incentives (mainly taxes) and regulatory burden faced by the supply side of the economy, assuming that the barrier to faster economic growth lies on the supply side of the economy.
Although during the election campaign in 1980 President Reagan had promised to balance the federal budget by 1984 and rev up the economy just with tax cuts that, through faster economic growth, would be self-financing, in fact his administration coupled the huge cuts in the individual tax rates it got swiftly passed by Congress with huge increases in defense spending and even farm support, driving up federal deficits to levels easily three times as high as the previously much decried, relatively puny deficits registered by President Carter (see chart below). By the end of President Reagan’s eight-year term in office, the public federal debt had tripled. By the time President Bush Sr. left office, it had quadrupled.
Had President Reagan really tried his hand at supply side economics, he would have lowered substantially the corporate tax rate from the statutory level of 35% to closer to 20% or even below, to keep U.S. capital and investments at home. Instead he left the high statutory corporate tax rate in place and even increased the tax take from the corporate sector by closing some loop holes. Reagan’s tax policy – especially his second-term efforts to close loop holes and broaden the tax base — actually seemed to slouch toward policies many Democratic economists would and did support. The point here is that overall, one can fairly argue that Reagan’s fiscal policy slouched much more toward the much maligned Keynesian policy of driving economic growth, rather than to solid supply side economics.
Seemingly paradoxically, corporate executives tend to go along with cuts in individual rather than corporate tax rates. It is so because they all manage two companies: one owned by shareholders, and the other, increasingly large company owned by their families. When given a choice between tax cuts for either or the other of the two entities, they naturally lobby for the second, which is what Republican presidents – Reagan, Bush Sr., Bush Jr. — have always faithfully delivered. We shall see what President Trump will do in that regard.
The CBO graph above also shows the eventual decline in the federal deficit and emergence of a federal budget surplus under Democratic President Clinton (although in fairness it must be said that then House Speaker Newt Gingrich gave him a helping hand). When President George W. Bush ascended to the White House, he actually inherited a federal surplus and the prospect of shrinking public debt. His fiscal policy frittered away both.
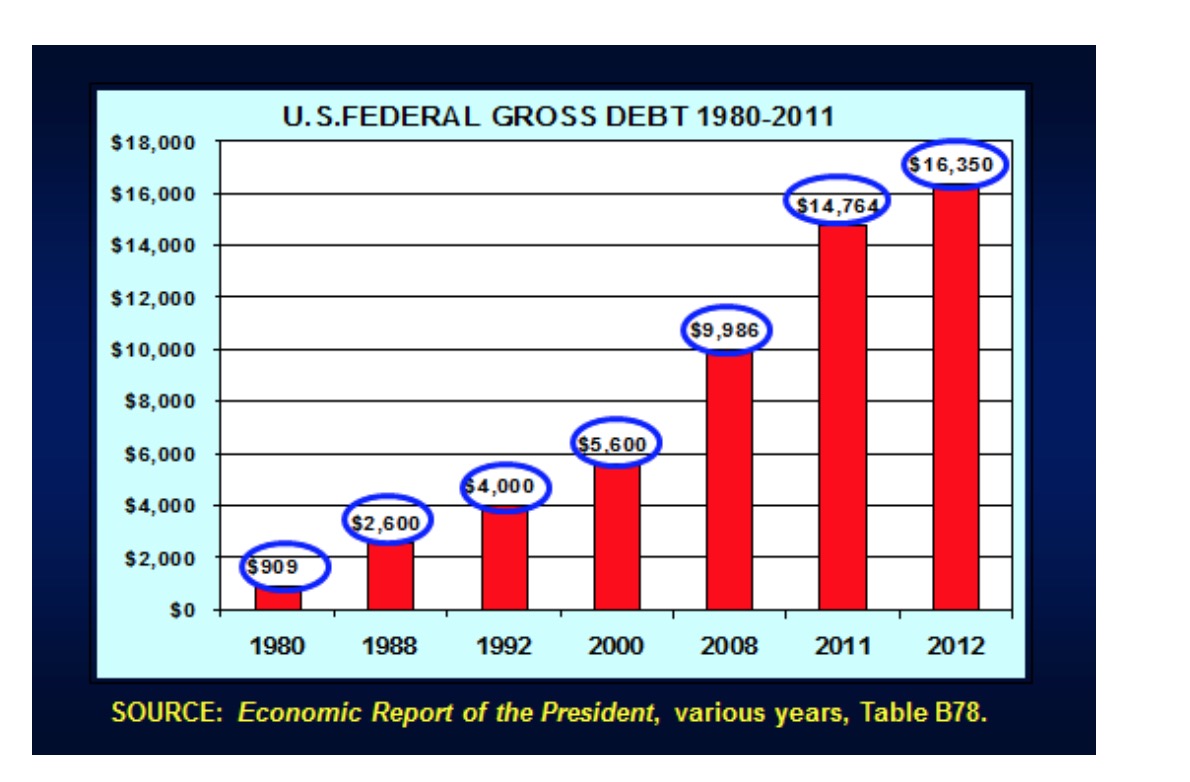
President George W. Bush, starting in 2001, basically repeated the rather reckless Reagan strategy of trying to goose the economy through increased government spending coupled with massive cuts in individual income-tax rates, all financed with large deficits and rapid increases in the federal debt. Under his reign the federal public debt rose from $5.6 trillion to close to $10 trillion. With the Medicare Prescription Drug, Improvement and Modernization Act of 2003, he even put a brand new future entitlement – heavily subsidized drug purchases by Medicare recipients – on the federal tab. That even after that action deficit financing of large future entitlements can so easily be hung around the neck of Democrats attests to the political power of the Republican oral tradition.
Finally, the CBO chart clearly shows that it would be unfair to impute the huge budget deficits and run-ups in the federal debt after fiscal 2009 to President Obama. In the wake of the global financial crisis of 2007-2009 – not of either President Bush’s or President Obama’s making — government revenues plummeted and much of the increased spending came from the so-called automatic stabilizers – mainly entitlements such as Medicaid, unemployment compensation, food stamps etc. – long ago baked into federal law. Neither of the two presidents had any control over these trends. Indeed, according to the CBO’s Budget Projections of January 2009 – published before President Obama had moved into the White House – the projected deficit in President Bush’s last budget, submitted in October 2008 for fiscal 2009 (October 2008 to September 2009), was close to $1.2 trillion. Surely that did not conform to the President’s idea of sound fiscal policy.
With this brief historical background, one can just see what might happen to fiscal policy under the reign of President Trump.
My hunch is that, to win a second term, he will heed Vice President Cheney’s dictum and, once again, practice the good old Keynesian economics that the American public loves so much: large tax cuts combined with massive, job-creating increases in federal spending on defense and on infrastructure projects, including, perhaps, sparkling new elementary- and high schools and perhaps even new health-care facilities in inner cities, to own up visibly to the folks living there to whom he had promised help, and all debt financed as good investments to make America grow and great again. Why not?
The alternative, asking the private sector to finance these infrastructure projects, may seem attractive to Republicans at first blush, but one must wonder how folks in the so-called “fly-over” country will react when all of a sudden their hitherto free roads and bridges are converted to toll-charging facilities, with tolls set on Wall Street by rapacious private equity firms beholden only to their equity investors in the US and abroad. It might not be a vote getter.
Keynesian economics has worked well for Republicans, because voters love it, as they seem to get something for nothing, federal debt and future taxpayers be damned. And in a world financial market awash in capital with nothing to do, safe U.S. government bonds will find many eager buyers.
It is all quite confusing, even to a Ph. D., and perhaps especially to a Ph. D., because, as I noted in the introduction, U.S. politics are ever so much more intellectually taxing than is the good old Slutsky Decomposition.
This week, as a fourth indictment came due, a tragic Donald Trump headed back to social media, digging himself into a hole that will eventually lead to some personal hell. But before Donald Trump, there was William Frederick Kohler.
He made his appearance on the American stage on February 28, 1995, an historian who had just completed his “Great Work” – The Guilt and Innocence of Hitler’s Germany. He was odd and dark and duplicitous. His life’s work was ready to go. All that was left was to write the introduction to his book. Instead his attention was diverted, as he followed his impulse to memorialize his own story dedicated to the “concealment of history beneath my exposition of it.”
Secretive and opaque, he was focused on a very special audience he labeled the “Party of the Disappointed People”, a group with whom he shared the affinity “that the loss has been caused in great part by others.” He hid the pages of the new and very personal (but incomplete) story from wife Marta inside the pages of the near completed Nazi history. And for some reason, he inexplicably headed to his basement and began to dig a tunnel to escape (or uncover) evil.
Kohler, like Trump, was not normal. Those who have analyzed his character describe him this way: “Preoccupied with evil, the nature of truth, and the effects of an individual’s relationship with others, he recalls his bookish childhood with a mother who drank to remember the ‘good old days’ and a bigoted father; graduate work in prewar Germany, where he hurled a brick on Kristallnacht; his unhappy marriage; and the lost love of his life, Lou, a former student. Kohler’s story exhibits the same inconsistencies and deceits he finds in history: Kohler, the personal memoirist … is as unreliable as Kohler, the eminent historian. A virtuoso performance without a grand finale.”
Kohler is the fictional creation of philosopher and novelist William H. Gass, author of the award winning novel, “The Tunnel.” The author is described in the opening line of his 2017 New York Times obituary as “a proudly postmodern author who valued form and language more than literary conventions like plot and character.” He died on December 7 of that year, at age 93, in St. Louis, where he had taught philosophy and linguistics for 30 years. Born in Fargo, North Dakota, he was translocated to Warren, Ohio at 6 months, and raised according to his own account by “an abusive, racist father and a passive, alcoholic mother.” These revealing personal details trace back to a writing style he developed and labeled, “metafiction,” or stories in which the author inserts himself.
Of more relevance to America’s current political dilemma is that Gass received his PhD from Cornell in 1954, in return for his dissertation “A Philosophical Investigation of Metaphor.”A metaphor, as we know, is “a figure of speech in which a word or phrase literally denoting one kind of object or idea is used in place of another to suggest a likeness or analogy between them (as in drowning in money).”
Gass’s love of metaphor is on full display in “The Tunnel”. You can almost hear the beloved high school advanced placement English teacher pleadingly asking her sleepy students “What do you think the tunnel represents?” Of the novel, one critic wrote, “As the novel progresses we see the lies, half-truths, violent emotions, and relative chaos of Kohler’s life laid bare, and while he continues to dig away at the memories of his past he also begins digging a tunnel out from the basement where he works, a reflection of his tunneling through himself.”
Beyond Gass’s own story line, and that of William Frederick Kohler, one can easily catch glimpses of Donald Trump. As he entered the strange world of politics, he embraced the use of metaphor with memorable 3 and 4 world phrases like “drain the swamp”, “the system is rigged,” and “take our country back.”
Andrew Hines, PhD, a specialist on the history of metaphor theory in the western tradition, traced the use of metaphor back to ancient times, to leaders seeking control of the “body politic.” Reflecting on Trump’s rise in 2016, he wrote: “In classical rhetoric, Aristotle even went so far as to say that the ability to discern these types of similarities was a sign of genius. As he saw it, a similarity between two things – a workforce and an army, say – can generate a new type of meaning for the listener. It can collapse all the complex problems and ideas together and thereby make them both intelligible and gripping.”
Trump mixes old, worn out “dead” metaphors like “take our country back” with occasional “live” ones. When he hits the mark, he makes news. For example, in a 2016 foreign policy speech, he used the metaphor, “shake the rust off American foreign policy” only to have it within days appropriated as a headline in the Financial Times.
Some have described Trump’s fragmented, sometimes confusing and incoherent style as “metaphorical chaos.” But Georgetown linguistics professor Jennifer Sclafani has suggested it is intentional, commenting that his speeches “may come off as incoherent and unintelligible when we compare it with the organized structure of other candidates’ answers. On the other hand, his conversational style can also help construct an identity for him as authentic, relatable and trustworthy, which are qualities that voters look for in a presidential candidate.”
Dr. Sclafani is the inventor of the term, “idiolect,” which she is careful to remind “is not the language of idiots, but an idiosyncratic form of language that is unique to an individual.” Nonetheless, she believes Trump’s style qualifies and works as authentic and relatable. His supporters, to deploy another metaphor, see him as “a straight shooter.” The problem for him now is complex. He has run out of targets who care what he says, and the hole he has dug has left him increasingly isolated even from those who fear him the most.
In the classic 2010 New Yorker article titled “Tocqueville in America” by literary critic James Wood, the writer picks apart some of Tocqueville’s less flattering observations about the nation he visited as a French aristocratic traveler in 1831. Considering the epic two volume “Democracy in America,” he prophetically lets loose with these words, “In the book’s second volume, he warns that modern democracy may be adept at inventing new forms of tyranny, because radical equality could lead to the materialism of an expanding bourgeoisie and to the selfishness of individualism… In such conditions, we might…meekly allow ourselves to be led in ignorance by a despotic force all the more powerful because it does not resemble one…”
Sadly, his words remind of another influential essayist, Kenneth Burke, whose 1939 masterpiece, The Rhetoric of Hitler’s Battle, is required reading for graduate students from English to Philosophy, and from Political Science to History and Religious Studies. The piece’s main focus involves a critical analysis of Hitler’s Mein Kampf (“my struggle”) which includes this stark warning.
Leaders of the free world need “to discover what kind of ‘medicine’ this medicine-man…concocted , that we may know, with greater accuracy, exactly what to guard against, if we are to forestall the concocting of similar medicine in America.”
Trump too has written his own fictional story; a despotic force with his own signature “idiolect”; as admiring of Nazism as William Kohler and as taken with sticky metaphors as William Gass in search of his own “Party of the Disappointed People.” Loyal indeed, like zombies, his followers and the Republican Party have followed him into the basement, and are heading down a tunnel which has no end. It has been “a virtuoso performance without a grand finale.”