Joining Matthew Holt (@boltyboy) on #THCBGang on Thursday July 27 at 1pm PST 4pm EST are Olympic rower for 2 countries and DiME CEO Jennifer Goldsack, (@GoldsackJen); patient advocate Robin Farmanfarmaian (@Robinff3); Kim Bellard (@kimbbellard); and medical historian Mike Magee @drmikemagee.
You can see the video below & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.
The concept of “centers of excellence” has been around for a few decades. Surely sending health plan members and self-insured employers’ employees to the best and most effective providers should improve health outcomes and save payers’ money? Sach Jain is CEO of Carrum which has been working on this problem, partnering with the best providers and aggregating that demand from employers…and putting it all on a state of the art platform. As you might suspect, it’s not as easy as it looks. Carrum raised $45m from Omers Ventures a few weeks back, on top of a decent raise from Tiger Global a couple of years back. So are they getting it right? Sach told Matthew Holt that they are for sure on their way….
Robert Frost once said, “Home is where, when you have to go there, they have to take you in.”
Increasingly, in our struggling society, that place is your local full service community hospital. During COVID, if it wasn’t your local hospital standing up testing sites, pumping out vaccinations and working double overtime helping patients breathe, we would have lost several hundred thousand more of our fellow Americans.
But it wasn’t just COVID where hospitals leaped into the breach. As primary care physicians’ practices collapsed from documentation overburden and chronic underpayment, hospitals took them in on salary. If it wasn’t for hospitals, vast swatches of the northern most three hundred miles of the US and large stretches of our inner cities would be a physician desert. Hospitals subsidize those practices to a tune of $150k a year to have a full service medical offering and keep their own doors open.
As our public mental health system withered, the hospital emergency department (and, gulp, police forces). became our main mental health resource. Tens of thousands of mentally ill folks languish overnight in hospital observation units because, despite not being “acutely ill”, there is nowhere for the hospital to place them. And as our struggling long term care facilities withered under COVID, those mentally ill folks were joined in observation by seriously impaired older folks too sick to be cared for at home. As funding for public health has withered on the vine, hospitals have become the de facto public health system in the US.
In a responsible society, those public health expenses would be funded directly as a system of social care, or paid for by local tax levies. In the system we have, paying for all this rests on hospitals caring for a small number of privately insured patients. Their health coverage pays hospitals rates in excess of the actual cost of care for the covered and relatively wealthy folks in the community. Private insurance is the real safety net in a health system which lacks both universal coverage and a commitment to public health as a social responsibility. This is where the controversy over permitting more physician owned hospitals comes to rest.
There are over a \ hundred physician owned hospitals in the US. Their number was frozen by the 2010 Affordable Care Act (aka ObamaCare), over concerns that increasing their number would destabilize our health financing system. This prohibition is being challenged 13 years later by folks who believe the “competition” between hospitals is good, regardless of the downstream consequences, and would thus reduce society’s cost of care.
Not all physician owned hospitals are alike. Some have emergency rooms and take all comers. Most do not. Some service a full range of the community-regardless of their insurance coverage. Most do not. Rather, most physician owned hospitals focus on providing privately insured folks elective imaging, surgery and other forms of intervention that generate large margins at relatively lower unit costs than the local community hospital. Physician owners get paid twice- once when they render the care, and again when they collect their partnership dividends at the end of the year, creating a compelling incentive to treat the marginally necessary cases. Caring for the “worried wealthy” is a much more profitable business than caring for the poor or the multi-functionally impaired chronically elderly. It is also cleaner, whiter, more orderly and less disturbing to patient ambience. You won’t find a lot of them in our inner cities, or for that matter, working class neighborhoods, let alone in small rural communities, Catering more or less exclusively to the privately insured is actually “skimming the cream” which provides the vital nutrients to the local community hospital.
The smaller the community hospital, the more damage that cream skimming does.
Perhaps a thousand rural hospitals are dangling by a thread post-COVID, and the loss of any of their patients to “exclusive” physician-owned facilities thirty or sixty miles away may be the difference between life and death for the hospital. So the idea that “competition” from physician-owned hospitals will force community hospitals to lower their costs is a toxic illusion.
Have circumstances changed in the thirteen years since ACA froze the development of physician-owned hospitals? Yes, circumstances have markedly worsened. Despite ACA and COVID era coverage expansions, in 2022, hospitals in the US faced the worst economic crisis since Medicare and Medicaid were create in 1965. Some have recovered so far in 2023, but many have not. The smaller the hospital, the harder it is to find clinical staff, purchase needed supplies and pay their bills.
It is difficult to imagine a worse time to siphon off the tiny number of privately insured elective patients that cover the cost of hospitals’ staying open. Re-opening the ACA’s ban on physician-owned hospitals would markedly worsen the economic circumstances of struggling rural and urban safety net, and damage the public health.
Jeff Goldsmith is President of Health Futures, Inc. and a long time THCB Contributor.
On one of the Sunday morning news programs Governors Spence Cox (UT) and Jared Polis (CO) promoted the National Governors Association initiative Disagree Better. The initiative urges that we practice more civility in our increasingly civilized political discourse. It’s hard to argue the point (although one can question why NGA thinks two almost indistinguishable, middle-aged white men should be the faces of the effort), but I found myself thinking, hmm, we really need to do that in healthcare too.
No one seems happy with the U.S. healthcare system, and no one seems to have any real ideas about how to change that, so we spend a lot of time pointing fingers and deciding that certain parties are the “enemy.” That might create convenient scapegoats and make good headlines, but it doesn’t do much to solve the very real problems that our healthcare system has. We need to figure out how to disagree better.
I’ll go through three cases in point:
Health Insurers versus Providers of Care
On one side, there are the health care professionals, institutions, organizations that are involved in delivering care to patients, and on the other side there are health insurers that pay them. Both sides think that the other side is, essentially, trying to cheat them.
Both sides think the other is making too much money and has become too concentrated.
This is a pointless battle, one that confuses the symptoms for the problem. The problem is that we know too little about what care is appropriate for which patients in what settings by which professionals, much less about who in the system are incompetent or overly avaricious. Solving that issue is perhaps the most important thing that everyone in the healthcare system should be focused on. If we knew those things, irritants like prior authorizations or claim denials would cease to be issues, not to mention that patients would get better care.
Disagreeing better would mean stop blaming the other side and start addressing the underlying problem.
Prescription Drug Prices
It’s no secret that the U.S. has long had the world’s highest prices for prescription drugs. Pharmaceutical companies claimed they needed those prices to fund innovation, and to subsidize those discounted prices in the rest of the world. They’ve played tricks like extending patient protections, even on drugs like insulin that are decades old. Their tricks led to the Lown Institute to create the Shkreli Awards, highlighting the year’s “most egregious examples of profiteering and dysfunction in health care,” naming the award after the disgraced pharmaceutical executive.
In 2022, Congress finally got around to allowing Medicare to negotiate price prices – for a small number of drugs – and the drug companies are responding as one might expect, “throwing the kitchen sink” in their efforts to slow or negate such negotiations. It would stifle innovation, and take away their Constitutional rights, they argue.
We were all (well, most of us) happy when drug companies quickly developed COVID vaccines, but it took $32b of federal spending to accomplish that, and, speaking of greed, we’re seeing problematic shortages of critical drugs because generic drugs aren’t as profitable for the drug companies.
The reality is that Medicare is pretty much the only major health insurance program (public or private) that hasn’t negotiated prices, and it’s shortsighted to expect that could be allowed to persist indefinitely. Meanwhile, we’re seeing drugs whose prices are in the millions of dollars range, and less than half of new drugs approved appear to be of substantial therapeutic value over existing treatments. This is a state of affairs that cannot persist.
Some drug companies bit the bullet when Medicare capped insulin prices, applying the $35 out-of-pocket limit more broadly, and the pharmaceutical industry need to be similarly thinking more about their public image – and the public good – when it comes to the forthcoming Medicare negotiations.
Disagreeing better would mean acknowledging that there’s “reasonable rate of return” pricing and there’s price gouging, so let’s find that line.
Abortion
This is perhaps the best example of disagreeing badly, and deserves an entire article devoted to it, so I’ll have to try to make my points succinctly. Look, I get that, for some people, the belief that life begins at conception is a moral or religious one that cannot be argued. It’s like the 19th century abolitionists believing slavery was wrong; thank goodness now for their stubbornness then against the tides of society at that time.
It should raise eyebrows that one consequence of abortion bans has been an increase in infant deaths. If we care so much about life, then our maternal and infant mortality rates would be much better. We’d also do much better about postpartum care, including ensuring Medicaid and other care, and would ensure adoption and foster care are viable alternatives. And we sure as hell would not be complacent about 11 million children living in poverty. It’s hard to see what religious or moral principles wouldn’t have as much fervor about these problems with as with abortion.
Disagreeing better would mean both understanding that trying to impose our beliefs on others should also include acknowledging their views, and recognizing that preventing abortions creates consequences that moral people cannot ignore.
————-
Politics impacts all of our lives, but often does so at a distance that many of us don’t easily recognize. Health care, though, impacts most of us directly and visibly, both in our health and in our pocketbook. Cynical as I can be, I still believe that most people in healthcare are trying to do the right thing, although sometimes they get confused about what that may be.
We’ve got to stop trying to find enemies in healthcare and start making allies, so that we can solve its problems. Disagreeing better is a way to start.
Kim is a former emarketing exec at a major Blues plan, editor of the late & lamented Tincture.io, and now regular THCB contributor.
Filling in the holes of recent stories in the New York Times, and Propublica on the outpatient care of patients with peripheral arterial disease
Most have gotten used to egregiously bad coverage of current events that fills the pages of today’s New York Times, but even by their now very low standards a recent telling of a story about peripheral artery disease was very bad.
The scintillating allegation by Katie Thomas, Jessica Silver-Greenberg and Robert Gebeloff is that “medical device makers are bankrolling doctors to perform artery clearing procedures that can lead to amputations”.
The reporters go on to tell a story about patient Kelly Hanna, who presented to a physician, Dr. Jihad Mustapha, in a private clinic with a festering wound. After being diagnosed with a poor flow to her leg that was likely contributing to the wound, Dr. Mustapha performed multiple procedures on her leg to improve blood flow in an attempt to ward off a future amputation. The procedures were unsuccessful, and Ms. Hanna ultimately did need an amputation.
The Times also briefly touches on some other patients of Mustapha who had bad outcomes. The majority of these cases appear to be related to complications patients suffered during surgeries. Multiple surgeons reported having to have done multiple procedures on Mustapha’s patients who had had complications. In 2020, the state medical board investigated Dr. Mustapha and referred him to the Michigan attorney general. An expert hired by the state medical board reviewed 8 cases and concluded the practice was characterized by overtreatment and poor documentation. Mustapha reached a settlement with the Attorney general where he was fined $25,000 but did not acknowledge any wrongdoing.
Mustapha questioned the expertise of the medical board that was overseeing him, and noted that any significant wrongdoing would have resulted in a much more significant punishment.
I’m sympathetic to Dr. Mustapha after reading the New York times article for a number of reasons. The claims of wrongdoing appear to stem from:
Dr. Mustapha is a high volume operator that does lots of limb salvage procedures and has been paid a lot of money for this.
Vascular surgeons at nearby hospitals had complained because they were seeing “a lot” of his patients having complications.
An insurance company reported 45 patients over a course of 4 years needed amputations.
Device companies that manufacture the tools used by physicians to open up arteries provide loans to physicians to buy these tools.
There have been many more attempts to open arteries that have taken place in private clinics since reimbursement rules changed.
This is all extraordinarily thin evidence to suggest wrongdoing on a grand scale.
First of all, the case the New York Times chose to present involved a patient with a wound due to poor peripheral blood flow from critical narrowing of arteries. Presenting with a wound like this is a very poor prognostic sign, and indicative of Chronic Limb-threatening ischemic (CLTI): a condition that carries a 1-year amputation rate of 20%, meaning 1 in 5 patients presenting like Ms. Hanna end up with an amputation. Dr. Mustapha, who also happens to be widely regarded as a pioneer in the PAD field, self-reported a 30-day amputation rate of 1.3%. This provides the appropriate context for the 45 amputations in 4 years reported by an insurance company. A successful, high-volume operator working with difficult cases is bound to have numerically more complications. Without denominators, “more complications” means little.
It is possible that Dr. Mustapha’s rate of complications look good because the patients being taken to the lab are lower risk patients who shouldn’t be in the lab having procedures done. However, there is little evidence presented to suggest that this is the case outside of anecdotes from disgruntled former partners who note they were pressured to refer patients for vascular procedures.
It is similarly challenging to know what to make of the complaints from neighboring vascular surgeons about complications in Dr. Mustapha’s patients. The surgeons are generally unhappy with other specialties managing PAD patients without their involvement, and they also don’t know the the denominator to know if the complications occurring are at a higher rate than what would be expected.
Unfortunately, and especially in complex patients, wires may break while doing procedures, and the only treatment at that point is a vascular surgeon. Again, without knowing the denominator of total cases, it’s irresponsible to suggest there is something deeply wrong going on.
The New York Times also accepts as fact the assertion from surgeons that more endovascular procedures lead to more amputations. While this may be true in individual cases of unscrupulous physicians, the national story does not support this claim. Despite the significant increase in the complexity and illness of patients that have been presenting with peripheral arterial disease, the rate of amputations has actually gone down, despite the fact endovascular interventions have rapidly increased.
While it’s possible to attribute the lower amputation rate to other improvements in wound care, the likelihood of this being the fundamental driver of fewer amputations over time is very low. At the very least, the graphs make it highly unlikely that the main contention of the New York Times article – that higher rates of endovascular interventions leads to more amputations – is true.
It’s unfortunate the New York Times screwed this story up so much, because there are real issues to consider in this space. There is little question that the financial incentives to find and treat peripheral arterial disease leads to inscrupulous operators that harm patients. Propublica does a much better job in their deep-dive into the PAD story which focuses on vascular surgeon Jeffery Dormu.
Jeffery Dormu was a double board certified vascular surgeon who was paid $13 million dollars by Medicare alone between 2013 and 2017. In 2018, he even opened a state of the art lab nicknamed “the Watcher” and was paid $18 million from Medicare in the next 3 years.
These payments made him one of the highest paid vascular surgeons in the country. The numbers reflected a high volume of care delivered but there were concerning indications much of the care delivered was unnecessary. Unlike the New York Times story that featured a patient with a non-healing wound that put her at high risk of losing her limbs, some of the patients featured in the Propublica article had mild symptoms. Propublica does a pretty good job diving into each patient story, but the US medical malpractice system is challenging for laypersons. Highly paid expert witnesses on both sides make strong assertions, and lawsuits are frequently settled because it makes the most financial sense to do so, not because the case itself may merit it. So its worth a closer look at the patients discussed
The first patient Propublica discusses is Mr. Rosenberg, an auto mechanic who sought out care from Dormu for increasing leg pain.
12.27.2016. Mr. Rosenberg meets Dr. Dormu.
A lower extremity arterial ultrasound revealed elevated velocities in the right proximal superficial femoral artery.
1.19.2017. Dr. Dormu performed an aortogram of the bilateral lower extremity with bilateral iliac runoff, which revealed a 90% stenosis of the right superficial femoral artery and 100% occlusion of all three tibial vessels. Based on these results, Dormu performed a percutaneous transluminal balloon angioplasty and a mechanical atherectomy and stenting of the right superficial femoral artery and stenting of the right superficial femoral artery. Dr. Dormu also performed a mechanical atherectomy of all three tibial vessels.
3.23.2017. In response to increasing severity of his leg pain, Dr. Dormu performed another angiogram. These studies revealed an 80% stenosis of the left superficial femoral artery and 100% occlusion of all three tibial vessels. Dr. Dormu performed a percutaneous transluminal balloon angioplasty, a mechanical atherectomy, a stenting of the left superficial femoral artery, a mechanical atherectomy of all three tibial vessels.
3.31.2017. Mr. Rosenberg presents to the hospital complaining of left foot numbness and coolness when laying down. He is again sent to Dr. Dormu, who on the same day, performs another angiogram which revealed an in-stent restenosis of the superficial femoral artery stent and a 60% stenosis of the tibioperoneal trunk. Dormu replaced the stent due to “recoil”, and performed another mechanical atherectomy and a percutaneous transluminal balloon angioplasty of the left superficial femoral artery and a percutaneous transluminal balloon angioplasty of the tibioperoneal trunk.
4.1.2017. Mr. Rosenberg again presents with leg pain. Dr. Dormu performed another angiogram which revealed an in-stent occlusion/restenosis of the superficial femoral artery stent and restenosis of the tibioperoneal trunk. Based on the results, Dormu performed a percutaneous transluminal balloon angioplasty of the left superficial femoral artery and tibioperoneal trunk. Another superficial femoral artery stent was placed as well. Dormu also sends Rosenberg to the hospital after this procedure for evaluation for bypass as well as a thrombolytic.
4.2.2017. A thrombolysis is performed in the hospital via a catheter.
4.3.2017. Rosenberg develops a large hematoma and a cold foot. Dormu removes the catheter and recommends an amputation.
4.8.2017. Rosenberg is transferred to another hospital for a second opinion. A CT angiogram shows a left common femoral dissection. No blood flow is seen below the mid thigh. All stents were occluded. On the same day, Mr. Rosenberg undergoes an above the knee amputation.
Dr. Dormu’s expert witness, Dr. Garry Ruben, said the interventions were warranted, and blamed Rosenberg’s course to not consistently taking anti-platelet medication that may have kept the stents open, and his preexisting medical conditions.
Mr. Rosenberg’s expert witness, Dr. Christopher Abularrage, a vascular surgeon at Johns Hopkins, disagreed. He found several “breaches of the standard of care.” : failing to prescribe conservative therapy and lifestyle modifications first, and persisting with “unindicated, endovascular interventions in the face of persistently poor outcomes and diminishing returns”.
It’s possible that Mr. Rosenberg did have severe claudication causing him to have pain at rest, and that he was appropriately diagnosed. There is little question, however, that there appeared to be no attempt to attempt to conservatively manage Mr. Rosenberg’s symptoms. Only 23 days passed between the initial meeting with Dormu, and the subsequent intervention on his leg.
The Maryland State Medical Board initiated an investigation in 2020 after a patient complaint that noted Dr. Dormu recommended an angiogram for severe itching in the legs. A second opinion from another physician at another facility resulted in a normal ultrasound. The itching turned out to have been a bad reaction to an insect bite. This and other patient complaints triggered a review of 11 patient records by two independent peer reviewers who found that not only were conservative measures not employed prior to progressing to more invasive procedures, but patients with normal diagnostic studies were also subject to invasive procedures with “no clinical justification”.
The cases supported the claim that Dormu was performing procedures with serious complications in patients that did not need them. Patient 6 could walk a mile prior to having symptoms. After a procedure with Dr. Dormu, the patient endured worsening symptoms and an inability to walk after the initial left leg arteriogram performed by Dormu. Dormu then continued to perform left leg arteriograms on Patient 6 despite worsening perfusion and more severe symptoms in that leg.
Dormu also appeared to misdiagnose individuals, incorrectly diagnosing Patient 10 with peripheral arterial disease, and then performing procedures that ultimately worsened lower extremity perfusion. In October 2022, the state medical board found him in violation of state medical law, citing, in part, his overuse of procedure. He was fined $10,000, his license was suspended and he was placed on a two-year probation, during which he must be supervised.
It does not appear Dormu has practiced since.
The story for Dr. Dormu gets even stranger. A press release from May 24, 2023 advertises a TV show medical drama that purports to be a retelling of the life of Dr. Dormu that references a past as a drug kingpin in Washington DC.
This hard-hitting retelling of Dr. Jeffery Dormu’s dangerous past as a former District of Columbia drug kingpin intersperses storylines from the doctor’s past and present. The series navigates his life and illustrates how one margin of error could mean the difference between life or death on the streets as well as in the operating room. From narrowly escaping life as a Liberian child soldier, organizing one of the largest gangs in DC history, the Gangsta Chronicles and becoming a drug kingpin, to attending an ivy league school, Dormu went on to win a civil rights lawsuit against four corrupt police officers. During the span of his career, he has surgically saved tens of thousands of lives and built the only black owned cardiovascular hospital in the world, a multi-million dollar facility. Margin of Error is a unique rags to riches story that will take fans on a multi-sensory journey.
The contrast between the New York Times story and the ProPublica story is striking. The New York Times chose to attack a well-respected pioneer of the field who does a lot of procedures that result in some patients having complications and needing amputations. The grievances about practicing below the standard of care come almost entirely from neighboring vascular surgeons with an axe to grind. A review from the State medical board and the Attorney general resulted in a fine with no admission of wrongdoing. His license was not suspended, and he continues to operate a busy practice today.
ProPublica showcased a vascular surgeon with a checkered past who clearly was unable to diagnose peripheral arterial disease appropriately and was doing a high volume of procedures on asymptomatic or minimally symptomatic patients. The investigation by the state medical board resulted in a suspension of his license, he does not appear to be actively practicing today, and the website for his vascular center is no longer available.
Both articles unfortunately leave readers with the impression that all endovascular interventions are suspect and are primarily driven by a need for profit rather than any desire to help patients.
Academic vascular surgeons who have been long banging the drum of overuse of endovascular procedures seized on these articles to call for greater regulation of vascular centers and the operators working at these facilities. Dr. Joseph Mills , President of the Society of Vascular Surgery encouraged vascular surgeons be involved in the decision making process for patients with peripheral arterial disease (PAD), and noted that very few patients with PAD actually should qualify for interventions.
But everyone involved with taking care of patients with PAD agree that critical peripheral arterial disease leading to amputation is a major problem that disproportionately impacts poor, black communities. Even the vascular surgery comment on the New York Times article ends with an entreaty to the media :
SVS urges media professionals to be diligent in presenting health care and medical information that is fully balanced, as coverage could lead to patient distrust and delays in necessary care with potentially adverse consequences.
Unfortunately, the pull for the salacious storyline that sells regarding greedy doctors hurting patients in the name of the dollar is too strong for most in the media to resist. In choosing the easy path to clicks, ignored are the real issues :
Medical training programs (funded with taxpayer dollars) that appear to rubber stamp the unethical and the incompetent. The egregious practice patterns of Dr. Dormu should raise serious questions of the programs that trained him (Vascular surgery specialization at Deborah Heart and Lung). Should programs and program directors responsible for signing off on trainees as competent to perform procedures independently face sanction when graduates of their program fail to do so?
If training programs are turning out some combination of incompetent and unethical graduates, the onus falls on state medical boards responsible for protecting the public from bad operators. The system appears to work in the case of Drs. Dormu and Mustapha, but the timeline for corrective action is too long. The first complaint reported to the Maryland medical board was in October of 2020. The resulting investigation and sanction to suspend his medical license did not take place until late in 2022. Two years of a dangerous operator like Dormu practicing medicine is too long.
The peer review process as a means of regulation appears to be highly susceptible to internecine squabbles that make it difficult to delineate right from wrong. Vascular surgery has a strong stance that has a protectionist bent to it. It is clearly in their interest to cast other specialties operating in this space in a poor light. Academics, especially, are hostile to all work being done outsie their purview. The currency in health systems is volume of procdures performed. Private clinics located in areas with a high prevalence of PAD threatens hospital volume. This makes peer review provided by vascular surgeons as a means of regulation suspect.
Atherectomy is controversial in part because the evidence in the form of clinical trials for their use is poor. More trials may shed light on exactly how inappropriate atherectomy is and define the population best suited for it.
Reducing or changing reimbursement for procedures in the outpatient/non-hospital setting is a common solution proffered by a number of commenters. Unfortunately, many of these commenters are in the academic hospital space and have much to gain from this type of regulation, and ignores the possibility that there have indeed been countless limbs saved by expanding access to those most at risk to revascularization.
This is certainly a good discussion worth having that deserves attention. The New York Times doesn’t appear to be the best place to moderate that debate.
Anish Koka is a cardiologist. Follow him on twitter @anish_koka
To listen to more of the discussion, tune in at 1 pm EST July 23rd on TwitterSpaces (Go to twitter and click on the pinned tweet on my profile @anish_koka )
Every time I get around to sending out the THCB READER I add a short & usually not to sweet commentary on some aspect of health care.–Matthew Holt
I saw the obesity crisis up close this week. And by that I’m not just referring to my addiction to Salted Caramel with Pretzel Ice Cream, bad though it is. Instead I felt thin because I went to Disneyland. But while I tip the scales at a BMI of 30 if I’m lucky, I genuinely felt that looking around Disneyland more than 50% of the crowd were obese and many morbidly so.
The rest of my trip to Southern California was quite a contrast because I’ve been watching a girls water polo tournament. Those young women and most of their families, as you’d expect, look very different. In this crowd I am definitely on the other end of the spectrum.
Obviously there’s a big socio-economic difference between the Disneyland attendees and a crowd centered around a sport largely played by rich, white kids. But at a time where we are arguing about whether Ozempic and its fellow anti-obesity drugs should be available via insurance, we seem to have no other strategies to fight the nation’s slide to obesity.
You’ve probably seen those photos of people on the beach in the 1960s where everyone is thin. I won’t claim to understand the science of what happened but clearly the prevalence of high fructose corn syrup and other highly processed food has much to do with it. As does the free rein food companies have had to advertise what are addictive products. I don’t know how we get to be a nation where everyone eats and exercises like a water polo player. But clearly we need significant changes in our agriculture and nutrition policies. We did it with smoking, so we know it can be done. If you don’t think we need it, I recommend a trip to Disneyland (and that’s the only reason I recommend one!)
Conclusion: For every hour physicians provide direct clinical face time to patients, nearly 2 additional hours is spent on EHR and desk work within the clinic day. Outside office hours, physicians spend another 1 to 2 hours of personal time each night doing additional computer and other clerical work. (Sinsky et al, 2016)
If we only had the tools and the administrative support that just about every one of us has been asking for, there wouldn’t be a doctor shortage.
The quote here is from 7 years ago and things have gotten even worse since then.
Major league baseball players don’t handle the scoring and the statistics of their games. They just play ball.
Somehow, when the practice of medicine became a corporate and government business, more data was needed in order to measure productivity and quality (or at least compliance with guidelines). And somehow, for reasons I don’t completely understand and most definitely don’t agree with, the doctors were asked not only to continue treating our patients, but also to more than double our workload by documenting more things than we ourselves actually needed in order to care for our patients. Even though we were therefore becoming data collectors for research, public health and public policy, we were not given either the tools or the time to make this possible – at least not without shortchanging our patients or burning ourselves out.
We didn’t sign up to do all this, we signed up to care for our patients. And we were given awkward tools to work with that in many ways have made it harder to document and share with our colleagues what our clinical impressions and thinking are.
It takes a lot of years to become a doctor, and sometimes many more years to become a good one. I don’t know whose harebrained idea it was to require us to do all the data entry to serve those other purposes that were never part of practicing medicine before. It has been said that seeing two more patients per day will pay for an assistant/scribe or whatever is needed.
So… Why is this not happening? In my own personal experience, we survived 15 minute visits with a previous EMR. With our new one (Epic, the probable industry leader), that is simply not possible. What’s wrong with this picture?
With clerical support, there wouldn’t be a doctor shortage and the burnout epidemic would not have the proportions it now has.
Let the doctors do the doctoring and leave the bookkeeping to someone else, at least until the EMR technology catches up and speeds us up instead of slowing us down!
Hans Duvefelt is a family physician, author, and creator of “A Country Doctor Writes.”
Joining Matthew Holt (@boltyboy) on #THCBGang on Thursday July 20 at 1pm PST 4pm EST are futurists Jeff Goldsmith; patient advocate Robin Farmanfarmaian (@Robinff3); Suntra Modern Recovery CEO JL Neptune (@JeanLucNeptune); and our special guest Investor at Bessemer Sofia Guerra (sofiaguerrar)
You can see the video below & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.
The All-in podcast is a fairly popular show that features successful silicon valley investors commenting about everything worth commenting on from politics to health. The group has good chemistry and interesting insights that breaks the mold of the usual tribal politics that controls legacy media analysis of current events.
Brad Gerstner, who is actually a guest host for this particular episode starts off by referencing something called Heartflow to evaluate the heart that has been recommended by one of the other hosts: Chamath Palihapitiya. Brad apparently asked his primary care physician about Heartflow and was instead directed to get a calcium scan.
Heartflow is a proprietary technology that purports to evaluate the presence of significant narrowing in the coronary arteries just by doing a heart CT scan. A calcium score is a low-dose CT scan used to identify the presence of calcium in coronary vessels.
The segment ends with a recommendation for everyone over the age of 40 to get some type of heart scan, so I thought it would be worth reviewing some of the main claims.
Question 1. Does Brad need a calcium scan?
Brad notes that his primary care physician told him he was young, fit, and had a low bad cholesterol (LDL) and needed a calcium scan rather than a heart flow scan. The answer to this question and the questions to follow depend on what outcome Brad is looking for. If the goal is to feel happier knowing if he has coronary calcium than the resounding answer is to get the calcium scan. But if the goal is to live longer and healthier, there is nothing to suggest a calcium scan will help. Most cardiologists believe that the lower the LDL, the better cardiovascular outcomes are. So if a calcium scan convinces Brad to NOT lower his LDL further either naturally or with medications, a calcium scan may be detrimental.
We have zero evidence to suggest patients who get calcium scans lower their risk of future mortality.
Question 2. Does Brad need a Heartflow scan?
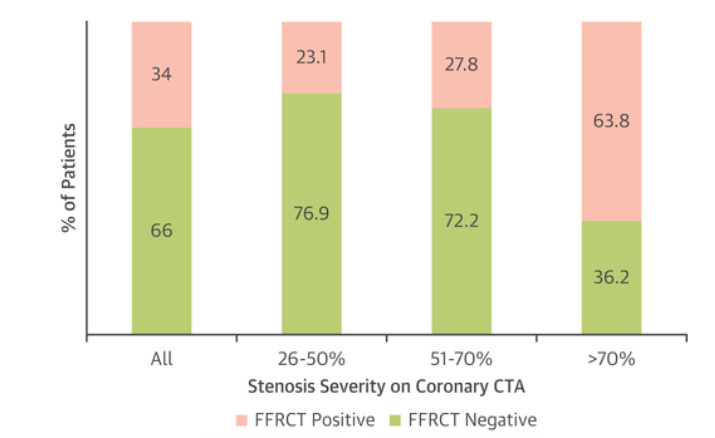
Heartflow is a California based company that claims to be able to identify heart vessels leading to a lack of blood to the heart muscle that need coronary stents to fix. Ordinarily this determination is done with a combination of tests that include a stress test and an invasive heart catheterization that involves a catheter being snaked into the heart. Heartflow puports to do all of this with a single 20 minute CAT scan that only involves placement of a peripheral IV using artificial intelligence/machine learning. The evidence to support the use of Heartflow comes mostly from small studies that show no difference in outcomes relative to the standard of care in relatively low risk populations. I could probably use a theragun based AI aproach in 500 carefully selected patients and show no difference in clinical outcomes to the standard of care. This is because the absolute risk of bad clinical events is too low for the size of studies generally being performed. You would need larger numbers to show small differences in outcomes and the Heartflow trials don’t have large numbers – which is convenient when you need series B funding. The small trials do still provide some interesting data about how Heartflow peforms.
The image below from this “positive” Heartflow study shows that almost a quarter of patients who did not have a significant narrowing in their arteries were judged to have a significant narrowing based on Heartflow. And regardless of whether you have a 26-50% narrowing or a 51-70% narrowing, you have a 1 in 4 chance Heartflow will say there’s a problem (when there isn’t).
So if Brad wants a pretty picture with some numbers attached to make him feel good, he should definitely pony up a few thousand dollars for a Heartflow scan.
Question 3. Will Heartflow or Calcium scans save lives if deployed broadly in the population?
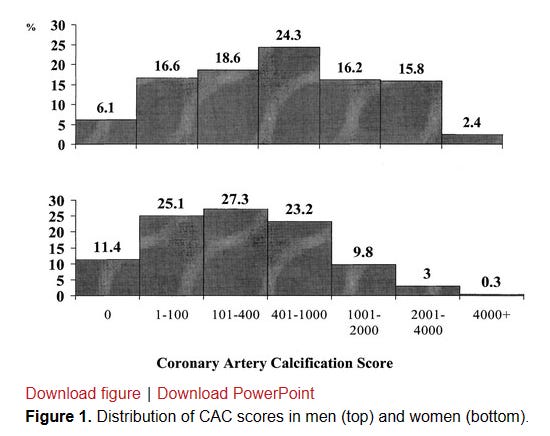
While it seems intuitively obvious that doing more tests to find heart disease will decrease the likelihood of dying from heart disease, the reality is anything but obvious. The history of diagnostic testing for coronary disease shows that we are better and better at identifying disease, but simply identifying coronary plaque isn’t the home run people think because of how ubiquitous the development of coronary plaque is in humans. By the age of 60 it is only the small minority of men and women who have no coronary calcium present (6% of older men, 11% of older women).
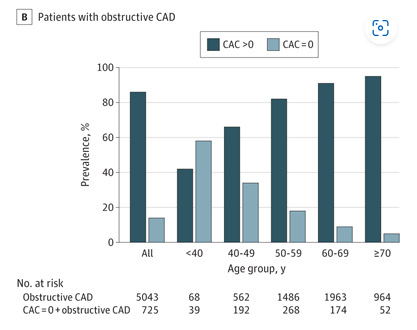
To make matters even more complicated, plaque in younger patients may be non-calcified and invisible to CT-calcium scans. A calcium score of 0 in a younger patient could provide a false sense of security. In the figure below, almost 60% of patients with “obstructive CAD” had a Calcium score of 0 !
Whether or not discovering and treating “obstructive CAD” as defined in the study is beneficial is another complex topic with much nuance.
And lastly, there’s a potential for harm driven by overdiagnosing coronary disease! Every cardiologist that has seen enough patients has a story of a patient with an elevated asymptomatic calcium score that ends up with a disastrous outcome from a cardiac catheterization. The field of interventional cardiology has a remarkable safety profile but the rate of severe complications related to the procedure alone is not zero.
Summary
Calcium scans and HeartFlow are interesting tools, but proponents are well out of their depth to think a universal screening approach using these tools will be beneficial.
The problem here is that these mostly middle aged men discussing the topic are appropriately concerned about the most likely cause of their early demise : heart disease. I’ve written a number of times about the scourge of heart disease in men. It can strike suddenly and without any warning, even in the apparently healthy. The absolute risk of men dying due to their heart giving out is ~ 1/600 in men aged 35-44, ~1/250 in men aged 45-54, ~1/100 in men aged 55-64.
This is enough death to strike fear into the hearts of the healthy, and provides ample opportunity to make billions selling men on the keys to cheating death.
If this topic piques your interest, and you want to dive even deeper, tune in tomorrow, July 16th at 1 pm EST to hear a discussion with cardiologists and other experts on Twitter!
Anish Koka is a cardiologist. Follow him @anish_koka on twitter.
Rough transcript of all-in-pod provided by YouTube:
1:31:50
about this pod is we cover everything from science to politics and and chamoth last year
1:31:56
um you know in his biohacking series told us all to get pre-nuvo scans which I did which is interesting and I think I
1:32:02
don’t know maybe 10 people have have sent you notes and said hey you helped me discover a tumor you know really
1:32:09
amazing well so this year and I did that um you know this year you’ve been talking a lot about heart flow so I said
1:32:15
to my general practitioner at my annual checkup hey I want to do this heart flow and she said oh you don’t need to do a
1:32:21
heart flow your ldls all your stuff looks real wait wait wait wait wait wait wait wait you have a female GP
1:32:27
uh she’s fantastic fantastic Stanford educated really terrific I don’t care
1:32:32
where she went who does the prostate test he does Hey listen it’s it you know
1:32:38
the perks that come check in the PSAs I mean no but seriously you have it really I do I do that’s a level of intimacy I
1:32:46
didn’t expect from you wow and so you know but what I found interesting is
1:32:51
when I suggested I get the heart flow she said oh you don’t need it Etc your ldls are low you’re very fit and she
1:32:59
said but on second you know maybe you could go get this calcium score test right
1:33:04
um I didn’t know anything about this but you know I did a little quick research and it turns out a big Jam of study in
1:33:10
2017 over 50 percent of men and women over the age of 40 Carrie plaque
1:33:16
plaque’s the number one killer it’s a source of heart uh disease and and heart attacks and as Chamas been talking about
1:33:23
there’s you know a a prophylactic called Statin which is basically like a supplement very little downside no
1:33:30
long-term downside effects but it immediately starts cutting down the amount of fatty cells and and and plaque
1:33:36
that’s carried in your blood so I thought it was interesting I went and I had chemath uh as you know the core the
1:33:42
coronary calcium scan it takes five minutes it costs between a hundred and four hundred dollars the fact that we
1:33:47
don’t have every person taking this over 40 is crazy and Frontline doctors should all be prescribed in it but it
1:33:53
particularly if there’s family history sorry but did you also do a contrast CT with heart flow yeah so I started with
1:33:59
the calcium score 150 bucks over at Stanford took five minutes and you know it told me uh you know which wasn’t
1:34:06
terribly surprising I was one of the 50 percent that did carry some level of calcium so it was called a non-zero
1:34:13
score and then what they suggest is because you have a non-zero score you get this
1:34:19
you know chamoth you told me go do the contrast CT which then will image what
1:34:25
this looks like actually in your artery so this past week in Boston I did the contrast CT again this took 10 minutes
1:34:32
non-invasive like you know it just they run you into it invasive because you have to put the dye so they put yes so
1:34:41
so a tiny bit I I suppose they shoot a little die into you but you know um uh it didn’t feel like anything
1:34:48
I was in and out of the of the place in 40 minutes and what it found is you know
1:34:54
fortunately that very little of this calcium had turned into what they call stenosis any narrowing of of the
1:35:01
arteries okay but then it gave you just a very clear picture that if you are one
1:35:07
of the 50 who carry plaque over the age of 40 you should be on a prophylactic
1:35:13
Statin so it’s chamat knows I signed up to 10 milligrams of crestar which I’m taking daily has had zero you know zero
1:35:20
adverse consequences and in two or three months they’ll test the amount of you know we’ll revisit this calcium score
1:35:28
um but when I talked to the head of Cardiology what was so interesting he said every one of his friends over the
1:35:34
age of 40 he has them do this calcium coronary scan it’s so cheap and if
1:35:39
they’re zero on their calcium reading that that’s the end of the line but if they have a non-zero reading then he’ll
1:35:45
do the the CT coronary scan which is again very cheap more expensive than the
1:35:51
calcium test but very cheap and when you think about the cost of the patients in this country right in our health care
1:35:58
System due to heart disease and when you think about the needless lives cut short I was shocked how easy all of this was
1:36:07
and how empowered I feel by the data and how fortunate I feel that I’m actually
1:36:12
taking a supplement I call it a supplement instead of statins because I think Statin has some spooky name it
1:36:17
sounds to me like a better supplement than any vitamins I can take and you know it’s reducing the ldls or these
1:36:24
fatties in your you know in your blood and I’ll keep you posted but I was very grateful and you know as you know I
1:36:29
posted it in our thread and I think all the besties you know we saw responses out of a bunch of folks in the thread
1:36:35
this week are going to go get their calcium uh you know coronary scan and I
1:36:41
I think it should be Common Sense on the front lines for people over 40 particularly if there’s any family
1:36:46
history go get this calcium test done this summer while you have a little extra time there you have it folks
1:36:53
100 to 400 could save your life calcium coronary scan Brad gerstner thanks so much for science Corner this week
As health care continues to move in the direction of unaffordability, policy makers are considering a range of options to bring down health care costs. The Health Affairs Committee on Health Care Spending and Value has identified four broad areas for reform, including administrative savings, price regulation and supports for competition, spending growth targets, and value-based payment. These measures appropriately target health care’s supply side and the excesses that exist in the health care system.
In this blog, I would like to highlight another avenue for savings: one that focuses on the demand side of the equation. It is possible to reduce health care expenditures by reducing the demand for care. This is distinct from rationing, which is the denial of needed care. I’m referring to genuine health improvements that make health care less necessary in the first place. This type of health improvement is the sweet spot of health care cost containment, benefiting both patients and purchasers.
In a previous blog, I posed the question: in an ideal world, how much would we spend on health care? I posited that in a perfect world, we would spend zero on health care because no one would be sick. While such a perfect world may be unachievable, having the goal in mind can serve to guide our way in the present moment—like entering a destination into GPS.
Measures that promote genuine health improvement can alleviate the burden of illness while at the same time reducing the cost of care. They move us in the direction we want to go. In this blog I provide several such examples.
An Ounce of Prevention
The CDC explains that there are several different types of prevention. Primary prevention happens prior to a diagnosis—for example, smoking cessation that is initiated before lung cancer develops, or seat belt use that prevents a car crash from doing any physical damage. This type of prevention occurs on a fundamental level—preventing the illness or injury from happening at all. Primary prevention promotes health improvement while also bringing down costs. However, the savings may be diminished depending on the level of health system involvement (e.g., if rather than quitting on his own, the smoker employs pharmacotherapy and counseling).
Secondary prevention involves screening to identify diseases that are occurring in early stages, before the onset of signs and symptoms (e.g., mammography and regular blood pressure testing).
Tertiary prevention involves managing disease after the diagnosis has already been made, to slow or stop disease progression. This includes measures such as chemotherapy, rehabilitation, and screening for complications (e.g., routine eye exams to detect and treat diabetic retinopathy).
Prevention has not always been shown to reduce healthcare expenditures. According to one report, “hundreds of studies have shown that prevention usually adds to medical costs instead of reducing them. Medications for hypertension and elevated cholesterol…and screening and early treatment for cancer all add more to medical costs than they save.” This reflects the fact that health care is expensive, and care can become costly, even when it’s implemented upstream. Such interventions may be beneficial, but they do not occupy the sweet spot of healthcare cost containment.
Twelve Steps
Alcoholics Anonymous now has over 2 million members in 180 nations and more than 118,000 groups. A Cochrane study pointed out that “alcohol use disorder (AUD) confers a prodigious burden of disease, disability, premature mortality, and high economic costs from lost productivity, accidents, violence, incarceration, and increased healthcare utilization.” In a systematic review of the literature, Cochrane found that “there is high quality evidence that [Alcoholics Anonymous/Twelve‐Step Facilitation is] more effective than other established treatments, such as [Cognitive Behavioral Therapy], for increasing abstinence.” Moreover, “AA/TSF probably produces substantial healthcare cost savings among people with alcohol use disorder.” This well-known health innovation is one that has been promoted and practiced by patients themselves, without the direct involvement of the health care system.
Prevention That Brings Down Psychiatric Hospitalization
I was diagnosed with bipolar disorder in 1998. From 2001 to 2008, I was hospitalized for mania at a rate of almost once per year (7 times in 8 years)—including one month-long hospitalization. In response, I developed from scratch a mood tracking system that was designed to help me monitor my condition and promote self-regulation. I used the system three times a day for a period of many years, and in doing so, I substantially reduced both my emergency room utilization and my rate of psychiatric hospitalization. This resulted in direct savings of tens of thousands of dollars. The intervention itself was free.
From 2008 to 2013, I was hospitalized at a rate of only once every three years. Today, I have been hospitalized only once in the past 10 years. I have not been hospitalized at all in the past seven years. These results point to the sweet spot of healthcare cost containment, where health improves and—as a direct consequence—spending goes down.
The mood-tracking system I developed was designed to flash red whenever I started to become manic. The system asks 10 questions (e.g., “are you feeling optimistic about the future?”) and assesses mood on a 100-point scale (anything above 50 is an up mood, anything below 50 is a down mood). My highest score was an 85, the day my son was born. However, I was not at all manic that day. So, I developed a second metric (on a 0 to 10 scale) that captured my mania level. On that scale, any score between 0 and 5 is a green light (not manic), 5 to 7 is a yellow light (caution), and 7 to 10 provides the red flashing light.
I found that having this early warning system enabled me to take steps to counteract the mania. For example, I learned that eating helps. Exercise helps. Talking to people helps. My therapist and I worked out an arrangement that, if I scored at or above an 8, and the system was flashing red, I would take an anti-psychotic pill PRN. These steps helped me to remain out of the hospital.
To generate the mania score, I asked 5 additional questions (e.g., hours of sleep, and number of “Big Ideas”). There was a measure for “outside warnings” (e.g., if a family member or friend expressed concern about my mental health). I quickly learned that this factor should be heavily weighted. The remaining two questions were for “caught manic thoughts” and “believed manic thoughts.” I might have thought that people were reading through my e-mails or monitoring my calls, but the thought was “caught” in the sense that I recognized it as manic thinking. A “believed” manic thought meant that the surveillance was really happening (i.e., I did not view my escalating concern as the product of mania).
Through trial and error, I was able to develop weights for each of these queries and I tabulated them in a formula in Excel. Over time, I was able to refine the weights until the scores gave me a highly accurate representation of my manic state. If the system says I am a 6.8 yellow, that is the correct depiction of my state at that moment.
But it was not just the output that proved helpful, it was also the process of inputting the data. The system forced me to monitor my own thought processes. I became acutely aware of my own manic thinking and then was able to take steps to counteract it. It was this process of self-regulation that allowed me to reduce the number of manic episodes I experienced—which reduced the number of emergency room visits and psychiatric hospitalizations I had to endure (at great expense to myself and the health care system).
Draining the Swamp
In 2022, the United States spent an astonishing $4.42 trillion on health care. Certainly, healthcare practitioners work hard to promote positive health experiences and outcomes, and their efforts should not be discounted. But I do not believe that referring to the health care system as a “swamp” is unfounded. Elliott Fisher and George Isham recently pointed out that greed plagues the system, saying: “the public impression that health care is largely about making money undermines the legitimacy and trust upon which we depend.”
The sweet spot of healthcare cost containment comes from draining the swamp, rather than trying to reform the swamp. Patients who do not require health care services do not incur health care expenditures. This type of demand reduction sidesteps other important issues, such as what psychiatric hospitals are charging for an inpatient stay, and what their quality metrics reveal. In an era of healthcare unaffordability, demand reduction is a direction we need to pursue.
Ben Wheatley has 25 years of experience working in health policy with organizations including AcademyHealth, the Institute of Medicine, and Kaiser Permanente (linkedin.com/in/ben-wheatley-05).