By KIM BELLARD
2020 has been an awful year. Hurricanes, wildfires, murder hornets, unjustified shootings, a divisive Presidential election, and, of course, a pandemic. Most of us are spending unprecedented amounts of time sheltering in place, millions have lost their jobs, the economy is sputtering, and over a quarter million of us didn’t survive to Thanksgiving. If you haven’t been depressed at some point, you haven’t been paying enough attention.
Within the last two weeks, though, there has finally been some cause for hope. Whether you want to credit Operation Warp Speed or just science doing what it does, we are on the cusp of having vaccines to battle COVID-19. First Pfizer/BioNTech, then Moderna, and most recently, AstraZenica, announced vaccines that appear to be highly effective.
We’re having our Paul Revere moment, only this time with good news. The vaccines are coming! The vaccines are coming!
It strikes me, though, that our enthusiasm about these vaccines says a lot about why the U.S. has had such a hard time with the pandemic; indeed, it tells us a lot about why our healthcare system is in the state it is. We’re suckers for the quick fix, the medical intervention that will bring us health.
Unless you were alive when Woodrow Wilson was President, COVID-19 has been the worst public health crisis of our lifetime. It took some time for us to fully realize how bad it was going to be, and, even then, most of us underestimated exactly how bad that would be. We may still be underestimating how bad these next few months will be.
We knew, of course, that we didn’t have any vaccine for this new virus, and that, at best, it would take some time to develop one. We didn’t initially know what to expect when someone became infected, didn’t know the right treatments, didn’t know which therapeutics might help. We weren’t even really sure how COVID-19 spread. There have been many hard-won lessons.
What we did know, though, was that we needed to take precautions. Physical distancing, limiting social gatherings, wearing masks, contact tracing; we knew these things would help. They wouldn’t prevent COVID-19 from spreading, they certainly wouldn’t cure it once infected, but they would mitigate.
We couldn’t even do those right.
Mask wearing became a political issue. It is not a coincidence that some of the areas with the lowest percent of people wearing masks are among the hottest spots for spread of COVID-19, such as North Dakota, which has the highest COVID-10 death rate in the world right now.
While overall mask wearing has improved from the spring, to the point as many as 90% of Americans claim they usually wear a mask in public, it varies widely, as illustrated below:
Similarly, business shutdowns and stay-at-home orders have faced great resistance, again more along political lines than to intensity of COVID-19 cases. There are no doubt grave economic impacts to them, as we’ve seen, but whatever such measures we tried in the spring are now seen as a price we are no longer willing to pay.
Of course, if we had quicker and more widespread testing, and better contact tracing, we might not need such extreme measures, but we’re not very good at them. We don’t have enough tests, they take too long for accurate results, and a sizeable number of Americans view contact tracing with suspicion.
The CDC pleaded with us to celebrate Thanksgiving at home with only the people we live with. Do we listen? Of course not; nearly 40% of us plan to attend large gatherings. Over a million Americans flocked to the airport yesterday – the highest daily number since mid-March – with millions more expected to travel between now and Thanksgiving. That is admittedly down from previous years, but at a time we are regularly breaking daily records for cases, hospitalizations, and deaths, it seems rather foolhardy.
Why should we worry? There’s a vaccine coming.
Of course, no vaccine has yet been approved, none is in full production, there are tremendous production and logistical issues to overcome. It will take many months to have enough supply to vaccinate enough people to make an impact on COVID-19’s spread.
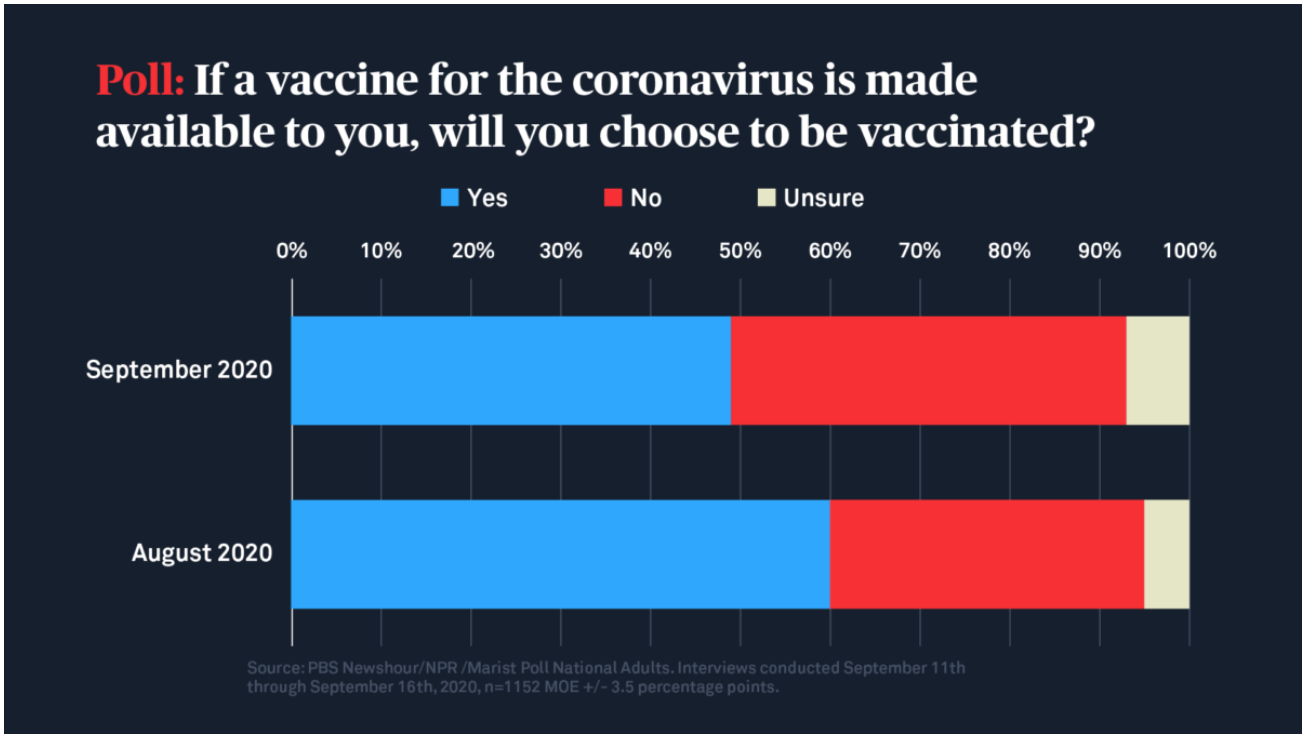
Equally troubling, experts estimate that, even with a vaccine that is over 90% effective, over 70% of people have to get vaccinated. That may be a problem; fewer than 60% of Americans say that would be willing – and that’s up from earlier in the year. Even healthcare workers, who are expected to be first in line when vaccines become available, are not yet convinced they’ll take it.
There may be a light at the end of this particular tunnel, but it’s a long tunnel.
We’ve all got pandemic fatigue, we all want COVID-19 gone, we all want to go back to our “normal lives,” but we don’t seem quite able to bring ourselves to do the things we should in order to help bring those about. Somehow, we assume, doctors and scientists will fix things for us. It’s par for the course.
We don’t do enough about our diet and exercise; it’s easier to just take pills for our high blood pressure and bad cholesterol. We don’t eat enough fruits and vegetables, so we take supplements to get the necessary vitamins and minerals. We don’t stay active enough, so we end up with hip and knee replacements. We claim to worry about the safety of vaccines, but give processed food manufacturers carte blanche to tailor their products to maximize our consumption.
We debate the need for universal coverage, but don’t spend nearly enough time talking about food or housing insecurity. We not only can’t persuade ourselves to take climate change seriously, we don’t even care to ensure that our water and atmosphere are safe now.
It’s easier to trust health care to protect our health than to take responsibility ourselves, even though medical care is estimated to only account for 10-20% of our health. So why wear a mask? Why social distance? Why stay in our family bubble? Soon there will be a vaccine. We need to stop acting like the proverbial damsel in distress waiting to be rescued, and start taking more responsibility for our own health – for COVID-19 and all the health issues we face.
Kim is a former emarketing exec at a major Blues plan, editor of the late & lamented Tincture.io, and now regular THCB contributor.
from The Health Care Blog https://ift.tt/2JdgNzO