Savvy health tech startups can learn how the differing investment priorities of venture capital funds and strategic investors (those tied to large healthcare organizations like health plans, pharma companies, and health systems) can impact everything from their capital raise to their ability to gain new clients. Brent Stackhouse, Managing Director at Mount Sinai Ventures, talks about the nuances of investing as a strategic, trying to balance a health system’s inherent aversion to risk with the gusto it takes to place good bets on the future of health. Where does a hospital system find investments? Are they looking for clinical solutions or consumer solutions? Brent shares the details behind Mount Sinai’s investment thesis and talks ‘big picture’ about trends he’s seeing in healthcare investing worldwide.
Filmed at Frontiers Health Conference in Berlin, November 2019.
The Primary Cares Initiative provides new value-based payment models aiming to enhance the delivery of primary care to promote efficiency and quality while decreasing healthcare costs. In the second part of this two-part series, we explore how eConsults directly support this new initiative across several key metrics.
Introduction
The Primary Cares Initiative aims to enhance the delivery of primary care through value-based payment models. In Part One of this two-part series, we broke down the five payment models offered through this initiative, including two performance-based models (Primary Care First) and three risk-sharing plans (Direct Contracting). Alongside previous programs such as Patient-Centered Medical Home (PCMH), the Comprehensive Primary Care (CPC+) program, and the Medicare Advantage Value-based Insurance Design (VBID), the Primary Cares Initiative represents the most recent push for enhancing primary care within health care systems.
Yet,
as programs such as these continue to emphasize primary care providers as a
locus of optimal care, the question becomes: how can primary care providers (PCPs)
best work within initiatives such as these to enhance care delivery efficiency
and effectiveness, and what kinds of services and technologies can support this?
eConsults represent a particularly promising way forward for PCPs to meet performance metrics. An eConsult is an asynchronous peer-to-peer telehealth platform through which PCPs can consult with a network of specialists. The PCP enters relevant patient information and a clinical question through a secure portal, and a specialist responds (often within a day) with a diagnosis, treatment recommendations, and other resources if necessary. This enables PCPs to treat patients directly and promptly, supporting primary care capabilities and improving healthcare outcomes for low- and high-acuity patients alike.
A continuing challenge in
maximizing the efficiency and effectiveness of primary care relates to
specialist referrals. As more health systems look toward creating PCMH models
and consider adopting new value-based payment models under the Primary Cares
Initiative, eConsult platforms will be instrumental in improving team-based
care coordination and communication. eConsults directly support the Primary
Cares Initiatives by maximizing primary care’s value in healthcare delivery,
having demonstrated direct benefits in terms of costs, outcomes, and both
patient and provider satisfaction
Reduced costs
When it comes to increasing efficiency under the Primary Cares Initiative, a crucial aim is to reduce costs—for both healthcare organizations and patients—without sacrificing quality of care. Empowering primary care clinics to retain patients and treat them within the offices of PCPs yields greater savings for all stakeholders. An eConsult cost savings analysis demonstrated that $75 billion is spent annually on specialist referrals in the U.S. based on the following data:
9% of ambulatory visits result in a specialist referral; one in three hospital discharges result in referrals to other care providers
$965 is the average total downstream specialist costs resulting from one referral
On average, more than 70% of eConsults have shown to replace routine specialist referrals. This drastically reduces costs associated with unnecessary specialist visits, labs and diagnostics, as well as downstream avoidable ED and office visits associated with waiting for specialist availability.
According
to PCMH FQHC Vista Community Clinic’s ROI calculations, numerous positive impacts on
healthcare costs have resulted from using the eConsult asynchronous telehealth
platform. “We can estimate the total annual referral costs saved are $2,019,600
based on 1,800 eConsults replacing a visit. […] Our total program savings—1,800
e-consults at the current eConsult fee—equate to $1,794,600.”
Improved outcomes
Immediate access to necessary care through
eConsult-supported primary care leads to improved patient outcomes by increasing
access to appropriate levels of specialist care.
Several studies on eConsult outcomes
have corroborated this:
In a subset survey from 1,743 eConsults, surgery yield (percent of ambulatory visits resulting in a scheduled surgical case) increased by 11% (p=0.07) compared to standard care in a one-year retrospective study
eConsults led to modified diagnosis in 15% of cases, and treatment plan change in 24% of cases in a one-year prospective data review of pediatric eConsults
In terms of clinical care outcomes, one study found eConsults reduced time to complete a hematuria workup by more than 50%.
Increased provider and patient
satisfaction
Access and outcome benefits of
eConsult use directly ties into metrics such as CMS Star ratings indicative of
patient satisfaction.
Star
Measures C22 (Getting Needed Care) and C23 (Getting Appointments and Care
Quickly)
Star
Measure C27 (Care Coordination (CAHPS))
Star
Measure C21 (Plan All-Cause Readmissions Healthcare Effectiveness Data and
Information Set (HEDIS))
Dr. Denise Gomez, Internal Medicine physician and Medical Director at San Diego FQHC North County Health Services (NCHS), comments on how platform usage strengthens the provider-patient relationship; “Patient satisfaction and provider satisfaction are coupled. When patients feel they have received quality treatment, mission-driven providers feel more satisfaction in their work.” By offering physicians more control over patient outcomes and restoring PCP confidence in delivering the most meaningful care to patients, physicians realize overall satisfaction benefits through eConsult use.
In addition, eConsults have shown
to provide relief from specific factors contributing to provider burnout. “Quality
time with patients increases PCP satisfaction,” says Gomez. “Immediate
specialty recommendations allow the physician to be more efficient, allowing
for more time with patients and improved overall satisfaction.”
Conclusion
Primary care has increasingly been recognized as the key to addressing many lingering issues within the United States patient population, and the Primary Cares Initiative offers new models to support leveraging primary care physicians to improve performance in terms of health care costs, efficiency of care, patient outcomes, and overall satisfaction. By implementing innovative asynchronous telehealth technologies such as eConsults–aimed to overcome access, quality, cost and satisfaction challenges stemming from the specialist referral system–PCPs gain a means to play an even more integral and active role in patient outcomes. eConsults facilitate right care at the right time in the right place thereby expediting treatment and drastically reduce costs, resulting in significantly better outcomes and satisfaction. This enables PCPs to improve on metrics vital to succeeding under such programs as the Primary Cares Initiative—and other such primary care-focused initiatives that are inevitably around the corner.
Chris Jaeger is the Advisor for ACO and Health System Strategy at AristaMD.
Bryan Roberts of Venrock, one of healthcare’s leading venture capital firms, weighs in with his view on the health tech market ‘state-of-play’ as we roar into 2020. With a track record that includes athenahealth, Illumina, Grand Rounds, Castlight, and Lyra Health, Bryan’s not a bad investor to ask when it comes to identifying the “next big thing” in healthcare innovation.
Filmed at J.P. Morgan Healthcare Conference in San Francisco, January 2020
If you are not an IKEA
fan, or haven’t been spending any time in Dubai, you may have missed the
chain’s marketing campaign to help promote its second store in the area.
Titled “Buy With Your Time,” customers got store credits for how long
they spent getting to the store.
Gosh, that’s something
that should make any self-respecting critic of the U.S. healthcare system perk
up. Count me as intrigued.
The campaign involved
checking the customer’s Google Maps’ Trip tab to determine how long it took
them to get to the store. IKEA benchmarked the average hourly wage in
Dubai, and converted the travel time into how much credit they’d
generated. It works out to about $29/hour, or $0.48 per minute.
Spend long enough getting there and you could get a free coffee table or even a
bookcase. Prices in the store include the equivalent time currency.
“Before the birth of this campaign, we realized two things: time is precious today, and many loyal IKEA customers spend a significant chunk of it visiting our locations, which are sometimes away from the city center. We think it’s only right to reward our customers’ efforts by repaying them for the time spent reaching us. It’s our way of helping the Dubai community make the most of every minute.”
It is believed to be the first time a retailer is letting customers use their time as a means of payment.
The campaign depends, of course, on Google Maps’ ability to track users’ movements, and for customers to allow IKEA to use that data. On the other hand, Google is tracking those movements anyway, so the least we should get for that tracking are some free meatballs.
“I think the promotion is brilliant–even if it is just a marketing campaign to promote a new store. Any time you can turn one of your biggest challenges into a win for your customer, that’s still a win. And it’s also a very creative use of technology.”
Simon Chandler was more skeptical, warning in Forbes: “the promotion is another step towards normalizing the idea that it’s okay to be watched wherever we go so long as we receive ‘free stuff’ in exchange.” Still, he concedes: “this promotion opens the door to a significant and profound change in how consumers purchase goods, and in how they relate to brands.”
The program seems to
have been a success:
I love this campaign for
a couple reasons. One is the concept that it recognizes that, yes, our
time is valuable, and not just in a lip service sort of way. The second
is that “money” is a broader, more elusive, concept than the formal
forms of currency that we usually use.
Healthcare should be
thinking about both of those.
Travel is often not a prime consideration in healthcare, with medical tourism and centers of excellence still not achieving mainstream status. We like our healthcare local, failing to recognize that, for most of us, local is far from the best care we could get. But what if, taking a page from IKEA’s campaign, the time we spend traveling to — and taking off work for — sources of higher quality care translated into credits that we could use to pay for that care?
More important than travel time is the waiting. I have railed before about how the healthcare system often treats our time almost contemptuously. As I put it previously, we wait to get appointments, we wait at appointments, we wait during appointments, we wait for results after appointments, and, if we’re in a hospital or nursing home, we spend most of our time waiting. Plus, of course, we spend inordinate amounts of time enrolling in our health insurance plan, waiting for claims payments, and, should you ever need it, on hold in customer service queues.
Healthcare should be
valuing the time we spend in the system waiting for something to happen.
Some parts of the healthcare system seem to track and report waiting time —
e.g., urgent care centers or emergency departments come to mind — but they
don’t seem to do much with that information. E.g., a three hour wait at
an emergency room doesn’t give you any credit off the big bill you’ll get for
that experience.
The healthcare system values the time of the people and things in it, not the people using it. Imagine how the incentives would be different if our time cost them money. Note, for example, Nicos Savva and Tolga Tezcan propose in HBR that payments for emergency room visits be tied directly to wait times.
We shouldn’t just be looking at giving wait times monetary value, but also explicitly valuing the kinds of behavior that keep us out of the healthcare system. This has been the goal of “wellness programs” for several decades, despite near-universal evaluations from objective observers (e.g., Rand or Song and Baicker) that they are not really effective.
It boils down to the
fact that we have an illness system, not a system of health, and so all the
monetary rewards revolve around dealing with how we treat those
illnesses. In the ideal health-oriented system of the future,
payment should be oriented to activities and people who keep us healthy, or
return us to the best health most effectively.
Imagine instead of paying health insurance premiums we accrue credits for our good health behaviors, which can be redeemed when we need some sort of intervention to maintain or improve our health. IKEA couldn’t have done its campaign without Google Maps, and we’re getting close to the kind of 24/7 tracking options that would allow for us to determine and manage such credits.
The problem will be that no existing entities in the healthcare system are really equipped (or incentivized) to administer such an approach, opening the door to new types of market entrants. Maybe we should ask the people at IKEA…
IKEA’s effort may just have been a clever gimmick to promote a new store in an isolated location, but there are lessons to be learned from it nonetheless. As Mr. Aten suggested, turning pain points for the customer into a win for the customer is, in fact, a win. If there is something that we can all agree on, it is that healthcare has too many pain points for its customers. The question is: how can we turn them into wins for those customers?
Kim Bellard is editor of Tincture and thoughtfully challenges the status quo, with a constant focus on what would be best for people’s health.
With a holistic mind-body approach to treating chronic back pain and COPD, Kaia Health is a digital therapeutics startup gaining a lot of attention from some really big players, including Optum Ventures (the venture arm of U.S. health insurance giant United Healthcare) which recently made an $8M follow-on investment to the startup’s Series A. What makes Kaia standout in a crowded field of digital health solutions focused on chronic pain? CEO Konstantin Mehl points to their proprietary tech, which uses a smartphone camera to provide real-time corrections to patients as they complete their physical exercises. As digital therapeutics like Kaia gain greater clinical validation and show widespread improvement to patients’ lives, Konstantin shares his hopes for the future of reimbursement for clinically-proven health tech.
Filmed at Frontiers Health Conference in Berlin, November 2019.
Swedish Healthcare seemed competent but a bit uninspired and rigid to me but my medical school class trip to the Soviet Union showed me a healthcare system and a culture I could never have fully imagined in a country that had the brain power and resources to have already landed space probes on Mars and Venus by the time my classmates and I arrived in Moscow in the cold winter of 1977.
The first time we sat down for breakfast at two big tables in the restaurant of the big Россия hotel near the Red Square, our two male waiters asked if we wanted coffee or tea and people started stating their preferences. The waiters shook their heads and put their hands up in the air. No, they couldn’t split the beverage order, they explained. We had to all decide on one beverage with no substitutions.
The restaurant obviously had both coffee and tea, and as far as I know, they cost about the same. The only thing standing between the tea drinkers and their favorite morning beverage (the coffe crowd won the popular vote) was convention and attitude. I don’t know if this was a policy set by the hotel management or a complete lack of service-mindedness by he staff, but my classmates and I felt as if we, the customers, did not matter.
(Writing this piece, I came across the news item that the Hotel Rossiya, once the biggest hotel in the world, was demolished in 2006.)
From that first morning on, everything I encountered felt dim, dark and repressive. I saw with my own eyes that Sweden’s degree of uniformity was nothing compared to the Soviet Union’s, which some of my classmates, communists and former Viet Cong supporters, had spoken well of before we got there.
During our stay I saw dilapidated hospital wards and surgical suites with antiquated medical instruments in scarce supply, which we couldn’t even all see because of a lack of scrubs and booties. We saw bare-bones ambulances staffed with underpaid specialist physicians, neurologists for stroke victims, for example. I thought being a doctor in the Soviet Union seemed like one of the most depressing things you could end up doing for a living.
I yearned for the freedom and optimism I had seen back in 1971, when as an exchange student I fell in love with America and a girl I met in my high school sociology class.
During my high school year here, I got the impression that almost everybody in America had a personal ambition, like making music, writing a book or starting a business. I saw a service mindedness I had not seen in Sweden, where years later I saw the epitome of that in a restaurant near the Arctic Circle that closed for lunch (for the staff) from 12 to 1 pm every day.
In America I also got the impression that the rules of society were not exactly cut in stone the way there were in Sweden. Due dates seemed a little flexible, rules seemed to have countless exceptions; even spelling of the American language seemed to offer a few individual choices.
Doctors in America were mostly in private practice. I didn’t see much of American healthcare that year, except the afternoon reruns of Marcus Welby, MD that I devoured. It ran from 1969 to 1976 and it solidified my vision of being a primary care doctor in America.
Fast forward twenty years, to 1991, the year the Soviet Union collapsed. The Planned Economy proved itself to be an unsustainable daydream of the social engineers of communism.
That year I had lived in this country for a decade. My work in a Federally Qualified Health Center, part of a safety net that offered subsidized or free care to people without health insurance, had shown me the inequalities and health hazards of “the other half” of American society. I felt proud to be part of such a clinic, providing equal access to everyone.
During the ensuing two decades, the Federal agencies that paid our grants and provided our preferred reimbursement rates started to micromanage what we did and how we structured our work. My original liberated experience of American healthcare turned into a sense that the bureaucrats mistrusted doctors and administrators of FQHCs so deeply that they had to structure our work for us.
The crowning event was when we all more or less had to earn recognition as “Patient Centered Medical Homes”, which at first sounded like we needed to make our practices Marcus Welby-like. Instead, PCMH was not really about nimbly meeting your patients needs but about creating rigid protocols that in fact made it hard to improvise. This was followed by many other initiatives that to a small or larger degree lacked firm anchoring in the reality of front line medicine and became virtual shackles for medical practices.
This hampering of improvisation in how you meet individual patients needs felt strangely familiar, and brought back memories of that cold December morning in Moscow:
Tea or Coffee, but not both.
Save one same day slot and qualify for easy access recognition, double book freely and fail the access parameter (no “protocol”).
And then when Uncle Sam wanted our “data”, presumably for better central planning some day, we were given grants to computerize our patient records with numerous qualifiers about how to use these computers. “Meaningful Use” broadly sounded like a good idea, except the technology was immature.
One example: Patient information about their medical condition, if generated by the EMR software, often amateurish and rudimentary, gives us Meaningful Use brownie points, but high quality handouts from sources like Up to Date, Harvard or the Mayo Clinic don’t count.
Another Federal shackle: Uncle Sam wants us to deliver comprehensive care, which includes screening for a growing list of clinical and societal issues, like depression, alcohol use, domestic violence, sexual orientation, food insecurity and so forth. If we don’t do all this, we lose brownie points. Consequently, we hesitate fitting infrequent visitors into our clinic schedules, because you can’t possibly do all that in a single visit for a sore throat, so we look better if that patient goes to a walk-in clinic – one ding on the Access parameter instead of numerous dings for all the other ambitious comprehensiveness requirements
I am sorry to report that the well meaning bureaucrats of the Central Planning Office are making American Primary Care feel more and more like the Soviet Union of Lenin and Marx where people mattered as populations, perhaps, but not as individuals. That is not the way Americans think. They don’t want to be told what to drink with their breakfast and they don’t want to be told what the agenda is for their next doctor’s visit.
Collapse or profound disruption seems inevitable.
Hans Duvefelt is a Swedish-born rural Family Physician in Maine. This post originally appeared on his blog, A Country Doctor Writes, here.
Molly Coye has spent more than two decades working to advance technology initiatives in healthcare, serving roles as diverse as the Commissioner of Health for the State of New Jersey, Chief Innovation Officer for UCLA Health, and now Executive in Residence for AVIA, which mentors more than 50 large health systems on tech selection, adoption, and implementation. With such rich experience working with healthcare incumbents, we asked Molly to size up the current class of innovators, technologists, developers, and investors bringing the latest health tech solutions to market. What have they gotten right? Where do they need to improve? “We’re not so good at cost of care and lack of access,” says Molly, who also sees potential for that to change thanks to the work of organizations like Health Tech for Medicaid and an increased focus on solutions that address the health needs of ALL patient populations.
Filmed at J.P. Morgan Healthcare Conference in San Francisco, January 2020.
As a Petersdorf Scholar-in-Residence at the Association of American Medical Colleges (AAMC) in 2002, Dr. Thomas S. Inui opened his mind and heart to try to understand whether and how professionalism could be taught to medical students and residents. His seminal piece, “A Flag In The Wind: Educating For Professionalism In Medicine”, seems written for today.
Nearly two decades ago, Inui keyed in on words. In our modern world of “fake news”, concrete actions carry far greater weight than words ever did, and the caring environments we are exposed to in training are “formative”—that is, they shape our future capacity to express trust, compassion, understanding and partnership.
Inui reflected on the varied definitions or lists of characteristics of professionalism that had been compiled by multiple organizations and experts, commenting:
“From
my own perspective, I have no reservations about accepting any, or all of the
foregoing articulations of various qualities, attitudes, and activities of the
physician as legitimate representations of important attributes for the
trustworthy professional. In fact, I find it difficult to choose one list over
others, since they each in turn seem to refer largely to the same general set
of admirable qualities. While we in medicine might see these as our lists of
the desirable attributes of professionalism in the physician, as the father of
an Eagle Scout I know that Boy Scout leaders use a very similar list to
describe the important qualities of scouts: ‘A Scout is trustworthy, loyal,
helpful, friendly, courteous, kind, obedient, cheerful, thrifty, brave, clean,
reverent (respecting everyone’s beliefs).’ I make this observation not to
descend into parody, but to make a point. These various descriptions are so
similar because when we examine the field of medicine as a profession, a field
of work in which the workers must be implicitly trustworthy, we end by
realizing and asserting that they must pursue their work as a virtuous
activity, a moral undertaking.”
Later in the report, he shared: “The processes of formation include experience and reflection, service, growth in knowledge of self and of the field, and constant attention to the inner life as well as the life of action. ‘Who am I becoming as I move towards this life of service?’” My good friend, Fitz Mullan, the inspiration for the Beyond Flexner Alliance focused on the social mission in health professions education, was quick to remind me some years back that an equally important question is: “Why am I becoming that?”
In the same year when Dr. Inui was doing his AAMC fellowship, John Iglehart, founding editor of Health Affairs, interviewed Steven Schroeder, who had announced his coming retirement as CEO of the Robert Wood Johnson Foundation. Schroeder said, “If physicians and nurses, who are central to the operation of the system, however care is financed, are dissatisfied and feel undervalued, I grieve for that system because that is a system in trouble.” Here we see a shift, away from “I” to “it”. It is the “system”, not an individual or even an individual’s teachers, that is “in trouble”. “Bad people or bad design?”, W. Edwards Deming might ask.
Here
is the troublesome question that underpins the need for “Advanced Professionalism”:
What if our failings in ‘professionalism’ are more fundamental and foundational?
Might they be the result of a non-adaptive and ancient system – still centered
on a brick and mortar “hospital-medical office loop”; still backward facing and
reacting to illness rather then forward-facing and managing customized and
personalized strategic health planning; still over-investing at the tail end of
life and under-investing in conception to age three; still unaware that the
home could be a center of health and the care team could have (should have) a
24/7 health professional presence in it?
What if our mentors are able to “voice” and “model”
professionalism, and even appear to be “practicing” professionalism, but the
system itself makes it impossible for them and for their students to “realize”
true professionalism?
The role of ‘professionalism’ in training of physicians and in the delivery of care has been heralded by major scientific bodies including the AAMC, Institute of Medicine, the ACGME and the ABMS. Their listing of desirable attributes in health care professionals is helpful. However, what Fitzhugh Mullan understood was that—absent the context of rapid environmental change, the modeling of new approaches to care that are emerging from both the consumer and provider side, and the integration of the latest social science concepts which impact human planning, development and potential—physicians will predictably under-perform in the modern world.
What does Advanced Professionalism require? “Who am I becoming?” must be accompanied by “What am I building, where, how and for whom?”
Mike Magee MD is a Medical Historian and Health Economist at the Presidents College at the University of Hartford.
The shift in thinking required to go to a “virtual first” healthcare system may not be as unique to the health industry as we think. Teladoc Health’s new Chief Engagement Officer, Stephany Verstraete, got her start at Match.com — and explains the parallels she sees between the mainstream adoption of telehealth and what she experienced introducing online dating to the masses. Think about it: overcoming skepticism, addressing privacy concerns, and what Stephany says is most important, changing an ingrained behavior — are all challenges currently being faced by virtual care co’s. It’s not a bad idea to flirt with as we talk bigger trends in telehealth engagement.
Filmed at J.P. Morgan Healthcare Conference in San Francisco, January 2020.
Since Saturday’s Nevada primaries, confusion seems to be reining about how Bernie Sanders seems to be winning. Time (and not a lot more of it) will tell who actually ends up as the Democratic nominee. But the progressive side (Bernie + Warren) is doing much better than the moderate side (Biden/Butt-edge-edge/Klobuchar) expected, while we wait to see how the Republican side of the Democratic primary (Bloomberg) does in an actual vote. The key here is the main policy differential between the two sides, Medicare For All.
Don’t get too hung up in the details of the individual plans, especially as revealing said details may have hurt Elizabeth Warren. But do remember that there is one big difference between Sanders/Warren and the moderates. It comes down to whether everyone is in the same state-run single payer system (a modified and expanded version of Medicare) or whether the private employer system is left as it is, with expanded access to something that looks like Medicare (the public option) for everyone else. Note that no Democrat wants to stand pat on Obamacare “as is”. Everyone is way to the left of what Obama ran on in 2008 (or at least what he settled for in early 2009).
About 3 years ago as the dust was clearing from the Obamacare implementation, the impact of this started showing up in the polls. In 2017 for the Health 2.0 conference, Indu Subaiya & Hiliary Critchley ran a poll on health policy with Zogby. To me by far the most remarkable feature was that even though Obamacare was by then more popular than not among the public, the support for single payer had gone up dramatically since 2009–in the depths of the recession.
Zogby poll for Health 2.0, Fall 2017
In 2019 44% said they were utterly opposed to single payer (and 50% opposed overall). But by 2017 while the number strongly in favor had just edged up, 48% were in favor overall, with another 30% neutral or not sure. Now only 19% were strongly opposed.
Meanwhile, just a year later (October 2018) a lot of fuss was made about a poll from The Hill that had 70% of Americans supporting Medicare For All. This was the poll that had 52% of Republicans saying they were in favor of it. (Full data here). Don’t forget that only about 30% of Americans identify as Democrats, while about 35% identify as Republicans and 40% say they’re independent). So if we are to believe that somewhere between 45% and 70% of Americans say they are in favor of single payer, almost all Democrats are. And in fact that is true. The Hill found 92% were and the Kaiser Family Foundation (KFF) shows 75%.
The issue of course is what “Medicare For All” means in reality. The KFF poll is very up to date and I can’t decide if it shows that the electorate is very confused or if the poll itself is a mess. (I highly recommend clicking though it). It basically says that Democrats want Medicare For All and want a public option while wanting to keep their own insurance (presumably many of them now have employer-based private insurance).
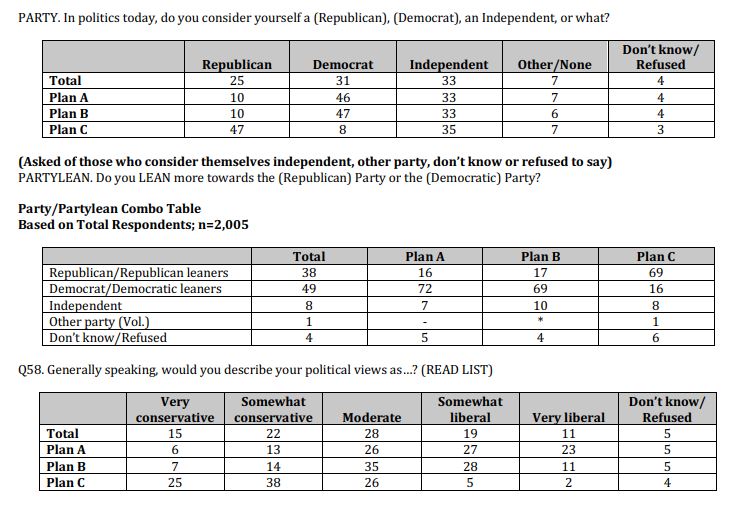
But luckily there was another recent poll done by Bob Blendon at Harvard (who I worked within the 1990s), and (as I told the KFF folks and Topher Spiro on Twitter) this poll was not a mess. In fact it was crystal clear in herding its respondents into one of three camps and thus very instructive for the Democratic primaries. (Details here) The poll gave people a straight choice between single payer, or extending the ACA, or the Republican “alternative”.
Basically when you tell Americans that Medicare For All means “Medicare for You too” (i.e. All Americans would get insurance from Medicare), but offer them a choice of an ACA expansion, roughly a third choose either alternative.
Somewhat more remarkably this split is not just along party lines. Democrats in the poll were also evenly split between Plan A (Medicare for All) and Plan B (expanding Obamacare) although few of them wanted the Republican alternative and, if you include independents who lean Republican, a third of them want single payer or extended Obamacare!
Source: Commonwealth Fund/New York Times/Harvard T.H. Chan School of Public Health, Americans’ Values and Beliefs about National Health Insurance Reform. July, 2019.
The inference is relatively clear. Almost all Democrats want Medicare (or something like it) “available” for All and about half of them (and about 1/3 of independents) are prepared to “mandate” Medicare For All.
How will that translate into the primaries? It’s relatively obvious that the most passionate and most progressive Democratic voters are a little more likely to vote in the primaries. I’ve cut some data from another poll from The Hill (Jan 15, 2020) that suggests that 58% of Democrats say they are certain to vote in the primary but 67% of liberals will, while only 50% of those who “lean liberal” will.
Question: How likely are you to vote in the Democratic primary election or caucus in your state to choose the Democratic nominee for the 2020 Presidential Election?
Which gets us back to the voting. Everything thus far is weird. Caucuses are stupid and unrepresentative, although they have elements of a good idea (2nd choice votes in multiple candidate fields). New Hampshire doesn’t look like America and neither does South Carolina. But with Sanders/Warren coming in at between 35% & 55% so far, and most more liberal and more activist Democratic primary voters favoring single payer, I suspect that we will see a majority of votes/delegates for Sanders/Warren by mid March assuming that health care stays the dominant and dividing issue.
That likely means that even if all but one of the “BBBKS” moderates drop out, there wont be enough moderate delegates to stop the progressives at the convention. (Worth noting here that Warren has been saying “Medicare For All after we fix Obamacare” which gives her a little slack).
If that’s right and Sanders is the nominee, then the Democrats face an interesting problem. If like 2018, they can run on how evil Trump and the Republicans are on health care, but not say too much about their own plan, then they’ll likely win. If Trump succeeds in making it all about single payer socialism making people fear the devil they don’t know, it’s likely to be a losing issue.
Matthew Holt is the publisher of THCB and likes to remind people now and again that he has a Political Science degree and worked for a pollster once!