For healthcare leaders who are “committed to community and career happiness” there is the Advancement League, a membership org dedicated to helping create the right circumstances and connections for both. Co-founders Alex Maiersperger and Antwan Williams tell us about the career development activities Advancement League has become known for, how they’re helping healthcare professionals at all levels of their career, and why their emphasis on community impact is important to anyone with a healthcare role. From ViVE 2022 in Miami, we also talk about getting together for Advancement League’s signature event, Young Health Leader Summit in Raleigh, North Carolina, on August 3-5, 2022.
This episode of Health Tech Deals is brought to you from the parking lot of a MacDonald’s in New Mexico. Yes, Jess is driving cross country from Florida! She and I hash out some health tech deals that happened this week: Brightline raises $105 million; Brightside raises $50 million; OssoVR raises $66 million; Podimetrics raises $41 million; and AmplifyMD raises $23 million.
This is the second part of former Kaiser Permanente CEO George Halvorson’s critique of Medpac’s new analysis of Medicare Advantage.Part 1 is here. The final part will be published on THCB later this week. Eventually I’ll be doing a summary article about all the back and forth about what Medicare Advantage really costs!-Matthew Holt
We clearly do have significant levels of quality data about the MA plans because we have extensive levels of quality programs and recognitions that exist in MA . Those programs get better every year — and MedPac should be reporting and even celebrating each year how many additional plans are achieving high scores in those areas as part of their report.
MedPac should be describing and celebrating progress that is being made in that five-star space and the members of the Commission don’t seem to know that information exists.
In fact, they sink lower than that pure denial in their report this year. They actually say in this year’s report that they have deep concerns about the quality of care for MA and they say clearly that they have no useful data to use for thinking about how MA is doing relative to quality issues.
Saying that there is no quality data about the plans is another MedPac falsehood (MPF) and, as they so often are, that particular falsehood is disproved quickly and easily by their own documents. In the final section of this year’s report where they were asked by Congress to do a report on the quality of care in the Special Needs Plans. The MedPac writers achieve that explicit goal in large part by using the easily available HEDIS quality data for those patients and for the other patients in the plans and by comparing both sets of numbers to relevant populations.
So this year’s report has that set of NCQA quality data for the MA plans included in it. MedPac is using it now even though they say no data exists and that means that’s another falsehood to say it doesn’t exist.
We know what the quality data of the five-star program is and we know what the HEDIS Scores are for the MA plans, and we also know how much MA costs us in every county because the bids give us that information.
We know that the plans bid below the average county fee-for-service Medicare costs in every county and we know what the total costs are by person for each county.
We need to know what the real costs are and we need to look at how we get the very best use of the Medicare dollar. MedPac should make it a priority to figure out how to get the best use of the Medicare dollar using both bids, capitation, and various kinds of ACO-related payment processes. ACOs all create better care than traditional fee-for-service Medicare, and the people who are critical of ACOs for not saving enough money should rethink their priorities. They should be happy with any use of the Medicare dollar that gives more for the member and patient
If an ACO that has team care and patient centered data flows just breaks even on costs relative to fee-for-service Medicare, that should be celebrated and supported as being a much better use of the Medicare dollar.
We should make patients our top priority. ACOs make patients their priority. MA Plans clearly set up benefits and care practices around the patient’s the top priority. Only fee-for-service Medicare completely lets the patient down by being rigid on benefits, rigid on service, and making costs a higher priority than people’s lives and doing that badly and inefficiently. We should be working through MedPac each year to see which approach to buying care actually gives us the very best use of our Medicare dollar.
How MA bidding works
The annual bidding process for the plans is important and it is not very well known to most policy people or to the news media in our country today. It directly anchors costs for every county for every MA member.
The plans each bid an amount in each county that will determine what they get paid in each county for each enrollee. They receive their capitation amount every month, meet the administrative and care delivery requirements that outlined in their MA contracts, provide all levels of needed care, and then they either make money or lose money on their bid.
That bid is a very powerful, important and relevant tool, because the capitation rate is the total amount that Medicare will ever have to pay for each MA patient. That cost control impact is an important point to understand. That bid and the capitation it creates actually caps costs and it defines costs for that patient.
Unlike fee-for-service Medicare — where the caregivers can and often do make much more money when their care fails because failures of their care in fee-for-service health care often increase the number of fees that are paid for a patient — the capitation rate paid to a plan is the full cost to Medicare for that patient and it can’t be increased in any way.
A congestive heart failure patient goes through pain, dislocation, and sometimes even fear of dying or fear of being permanently damaged when they have a congestive heart failure crisis — and the plans actually can save both money and save lives by not having those crises happen.
Those very same heart failure crises are often very profitable for fee-for-service Medicare care providers because they can and do generate from $20,000 to $40,000 in additional revenue for the care sites when they happen to occur for patients.
So, MA plans all build congestive heart failure crisis prevention protocols and fee-for-service Medicare does not even support or pay for the steps needed to put those processes in place.
So when the MedPac staff writes, as they actually do each and every year, that there is no fee-for-service quality data available and therefore they can’t comment on the relative or relevant quality issues for MA plans because those comments would be inappropriately unfair to the fee-for-service Medicare program, that is another inexplicable part of MedPac’s thinking. Their approach to reporting on MA should change before they write another annual MA report.
The actual impact of MA on people is ignored
They also inexplicably, unfortunately, and very completely ignore actual people in their MedPac staff annual report on MA .
They have no part of their annual report on MA that deals with the issues and the impacts of any of the actions or issues or processes on actual people and their lives. They have managed to write an entirely people-free report as their annual advice to Congress about the MA program. That does not seem possible, but it is clearly true and it is clearly intentional because the “people gaps” are so obvious and visible.
For example, Covid has just done damage to a lot of people in our country. Covid has been a major issue for people’s lives and for people’s care over the past couple of years. The MedPac report completely skips the topic of Covid impact on people except to speculate about whether Covid might have affected costs for either program in some way.
In the real world of people, there often were huge and obvious differences between the Covid responses of the MA plans and Covid responses of fee-for-service Medicare. A people-oriented annual report from MedPac on MA would have looked at those differences and pointed them out as very different uses of the Medicare dollar that happened down each of those payment pathways.
Every MA patient had a complete care-related contact system and support processes that were consistently and immediately in place. MA plans were recognized for being among the very first care sites in the country to have some of the Covid tests in place and they even sent nurses into homes to help with care very early in the process.
Every single MA member had the security from day one of knowing where to go for their Covid care. They all had care sites immediately because they were all members of plans, and those care sites and care systems in the plans all went through their own learning process to figure out the relevant Covid-related issues of care.
Fee-for-service Medicare had nothing.
Fee-for-service Medicare had no Covid plan or Covid-related approach. Fee-for-service Medicare left many people functionally orphaned and isolated because the fee-for-service enrollees who already had some level of care relationships in place could try to get into those sites but the people with fee-for-service Medicare Coverage who did not have care linkages in place were simply orphaned by Covid. They had to scramble on their own to find Covid care and information with literally no support from fee-for-service Medicare.
MedPac is supposed to be writing a report evaluating MA .
This year’s MedPac report should have led with a report and an update on Covid in those various settings and it should have included an informed discussion of what we learned in the process — and MedPac completely and carefully dodged the issue. It wasn’t even mentioned because MedPac does not mention or include people in their report in any case and it is also much easier to continue to be generically critical of MA if you leave people and their lives out of your analysis, research, thinking, and report.
How Medpac calcluates MA “costs”
What they did mention, in several places and in multiple pages of the report, was that they believed that MA capitation is too high and they stated that the capitation is more than Medicare would have spent for those same enrolled people if they had not enrolled in MA Plans.
They stated a couple of times that when they looked at how much fee-for-service Medicare would have spent paying for care “for those same exact enrollees,” it appeared to them that that number spent to buy each piece of the care that actually happened for those MA members was lower than the actual capitation that was paid to the plans for those exact same enrollees.
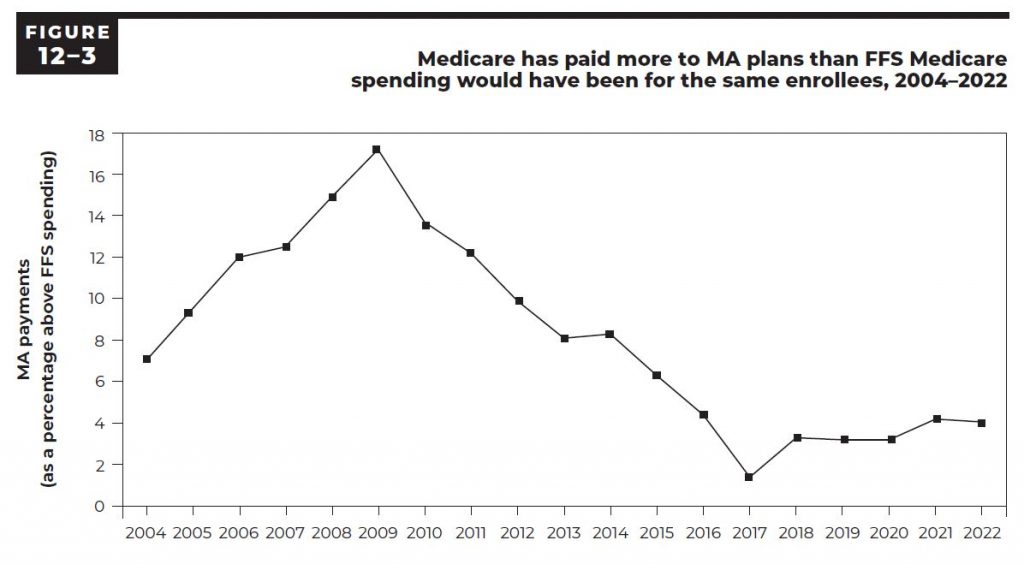
They estimated from that particular calculation that it cost about 4 percent more in capitation last year than Medicare would have spent buying those exact sets of Medicare services for those same patients if the people had not been enrolled in the plans.
They repeat that perspective and that conclusion several times. It’s also actually almost the only line chart in the entire report. Figure 12.3 (cut and reproduced below) has the number.
They run the numbers back to 2004 to show that the number has existed as a difference between those calculations every year and that the distance has been consistent over time.
That chart and conclusion gets quoted in multiple settings in health care policy circles as being basic context for whether the plans are overpaid and many people in both media settings and academic settings believe that number to be true and cite it in various places.
The problem with that number and with that calculation is that they very carefully price only the exact pieces of care received by those members and some of the most relevant pieces of care do not happen for those exact members because care is actually much better in MA plans. The capitation calculation numbers that create the baseline data and the bidding floor for each county are inclusive average numbers for the fee-for-service Medicare patients in each setting and they are based on and include the higher costs of poorer care that generally is delivered in fee-for-service Medicare.
The differences are easy to see and understand.
MA members have about 35 percent lower use of emergency rooms. They also have a significantly lower number of congestive heart failure related events. The fee-for-service care that was the basis for the capitation calculation and baseline number had all of those higher expenses built into them. That means that the only way that number from figure 12.4 can legitimately be used by MedPac to evaluate the relative costs now would be to add the relevant ghost numbers for those better care patterns back into the amount to show the cost that Medicare would actually have spent for those patients if they had not been enrolled in MA plans.
The MedPac staff clearly knows that those are fake and deceptive conclusions about the patterns of care and about the relative costs of the programs because they actually say very clearly in this year’s report — toward the end of the report in a discussion on another topic: “Plans steer patients away from an emergency department when an urgent care clinic or physician visit would suffice and is available.”
So even this report as written shows that they know that truth about those care pattern differences.
They very carefully tee up the illusion of a higher payment level for capitation each time by saying: “This is exactly what those exact same MA patients would have cost if their exact levels of care had been purchased by fee-for-service Medicare using the fee-for-service fee schedule.”
That is only legitimate information if they add to that cost number they compute for the current enrollees’ levels of care by putting those emergency room visits back into the cost total.
The average difference in costs of care that should be added back into that calculation to make the conclusion and to make the comparison with current members’ costs legitimate is actually about 9 percent additional costs — based on other available data. Without that 9 percent, this is false information and it is fake news.
How much do MA members actually cost?
What is true about the relative cost of care for people who enroll in MA ?
That is actually also relatively easy to see and know and it is also already embedded in this same report at several levels.
The bids are key.
The bid process and the numbers that relate to it already show us how much different the costs are for Medicare and for MA . The average area’s costs for fee-for-service Medicare are very legitimate costs. The bids then create the actual cost of MA measured in real dollars. The plans bid each year for every county and those bids both indicate what the cost differences are and what they have created in each county as the total cost each year to Medicare. We don’t need to guess or approximate or estimate the costs of the plans to Medicare because we now pay them in capitation each month. We don’t need to speculate about how much the plans might somehow cost us in total because the bids result in a capitation and because the capitation that is paid creates the actual cost and we know exactly what those capitation payments are.
So what are the bids?
The plans actually bid less than the average cost of care for fee-for-service Medicare in each of those areas.
The plans this year bid an average of 86 percent of the average Medicare fee-for-service costs in the counties.
That means that if nothing else changed, Medicare would spend 86 percent of what it spent last year to provide care in that county for those enrollees.
That initial bid isn’t the final cost. MA has what is probably the best quality assurance program of any government purchased care program in the world. That program includes a five-star process that tracks care and service and actually awards plans from one to five stars for their measured levels of performance, and then pays more money to the plans with more stars.
Those standards set by that program have a huge impact on American health care because so many care sites are involved in MA as their source of payments and patients and because so many care sites have done very intentional and explicit work needed to earn the stars.
Thousands of care sites linked to MA plans have a chance to do better on their payments and their cash flow if they manage the blood sugar levels of their diabetic patients well, and the care teams get better every year in delivering that care and making sure their diabetics have care teams focusing on their care and getting it right.
Diabetes is the number one cause of blindness in the United States. Diabetes is the number one cause of amputations in America and it is also the top priority and most damaging co morbidity for causing death from heart disease. It is a very good thing that we have a five-star program in MA that encourages large numbers of doctors and many care teams in many settings to provide better care for their diabetic patients.
Those MA quality programs sometimes also have an extremely positive spillover community benefit impact on all patients in a care site or a community because the doctors in each setting prefer to practice consistent care and that level of better care rewarded by MA tends to be extended to all of the patients in those sites and settings. Several studies have shown very positive quality improvement spillover impacts exist on high volume MA counties from those programs.
MA pays money for that to happen.
Higher scores on the five-star quality results can and do actually significantly increase payment levels for plans. Plans can earn up to 5 percent more dollars by having more quality stars.
That program has probably had the biggest improvement on care quality for large populations and for a wide range of care teams of any other single program in the world. It has actually changed care at levels we can see and track over time. Again — the evidence on how well that program is doing is hiding in plain sight.
When the program was first started, less than a dozen very high performing plans in the entire country earned five stars and very few plans even had four stars. Plans and care sites across the country have worked hard and very intentionally on those quality processes since that time and today we have reached the point where more than 70 percent of the MA members are now enrolled in four- or five-star plans.
That is a major and visible improvement. CMS appreciates that progress and CMS has done wonderful and increasingly effective work in encouraging and supporting those levels of performance improvement in the care sites,
MedPac, however, doesn’t even seem to know that this work exists. The MedPac commissioners don’t ever talk about those parts of the MA program in their meetings and they don’t seem to have any knowledge that those programs or measurements and culture changes for care sites that have roots in MA even exist.
It’s not damaging the country or the overall program for MedPac to have a high level of ignorance about those issues because the people who actually run Medicare for CMS do understand the tool kit completely and the people in those leadership positions at CMS understand and support the approaches and use them well.
The people who run CMS will probably enhance several pieces of that process at this point for the Special Needs Plans in very high impact ways, and care will improve for that very important population of people as part of that agenda and of that focus by CMS .
MedPac, by contrast, has an almost inexplicable void in that area in their thinking and in their annual report.
That avoidance of the quality issue is just wrong.
George Halvorson is former CEO of Kaiser Permanente
This is the first part of former Kaiser Permanente CEO George Halvorson’s critique of Medpac’s new analysis of Medicare Advantage. The rest will be published on THCB later this week. Eventually I’ll be doing a summary article about all the back and forth about what Medicare Advantage really costs!-Matthew Holt
MedPac just did their annual report on Medicare Advantage (MA) and they were extremely wrong on several key points.
The MedPac staff has a long tradition of being critical of MA, and they also, unfortunately, have a long tradition of being inaccurate, misleading, and consistently negative on some key points for no explicable or easily understood reason.
They achieved a new low this year by spending more than 20 pages of the report warning us all in detail about the upcoming cash flow distortions and coding abuses that they say are coming from a risk adjustment model and system that actually no longer exists in 2022 as a functioning system for our Medicare program — and they are also continued their distortion about Medicare overpayment of the plans by running an artificial cost number that functions only to deceive and not to inform and by using what is essentially a fake news number several times in the report.
Coding and Risk Adjustment
CMS has now officially canceled and retired the CMS Hierarchical Conditions Categories Risk Adjustment Model that has been used for almost two decades to calculate risk for plans. It is dead and completely gone for 2022 — and MedPac explained bitterly for more than 20 pages why it was a damaging approach and they somehow did not mention that it was now gone.
CMS has some very good thinking people who brilliantly took that whole set of coding linked issues off the table by making the system that was being potentially abused simply disappear.
MedPac wrote more than 20 pages in this year’s official report about MA complaining about that exact process and system and they didn’t mention that it was gone or explain why it was important to not have that data flow create the risk level information that we will now be using to get diagnostic information into the system.
The new approach for determining patient risk levels is fraud proof. There is no way to put wrong data into the information flow that they are now going to use to see and determine which patients are diabetic and which have heart disease or who has drug abuse issues for the risk discernment processes.
The impact on low income Medicare patients & union members
MedPac also had a major content deficit in their report and managed to leave the most important aspects of the work being done now by the plans to help offset some of the damage done to too many Americans who have been damaged by social determinants of health issues for far too long in their lives. MedPac also completely failed to report and discuss the important reality of the fact that we have now reached the point where two-thirds of our lowest income Medicare beneficiaries are all voluntarily in the MA plans.
They also left out of their report the fact that a significant number of union trust funds and a significant number of employer retirement programs that had made significant promises of retirement health care benefits to their retirees over the past decades are actually having those commitments kept, met, and even enhanced with the relatively new employer-sponsored MA plans that work directly with employer settings.
Five million people who might have had their retirement health care programs bankrupt, underfunded, or at serious risk have found a very strong safety net in the MA program — and MedPac does not think that development was important to understand and probably celebrate.
Anyone looking at the future politics and funding of the MA program will find both that overwhelming support for MA from our lowest income people and from our most well-connected employer retirement funds to be good and important to understand.
MedPac missed every bit of that agenda and set of accomplishments in this year’s report.
MA vs FFS during Covid and beyond
They also left Covid out of the report as a care-related issue and the clear difference between the two programs.
They failed completely to explain the huge differences in the care reality, the personal comfort levels, and the direct care availability for Medicare beneficiaries. Care and treatment in the MA plans were significantly better on all of the Covid-related issues versus that for those people who were abandoned, isolated, and completely unsupported by the total non-response from fee-for-service Medicare.
MedPac should have used this report to explain what we have learned in that process — but they did not have any portion of the report that related to the impact of either program on actual people.
Leaving the impact of the program on people completely out of the report is not a new trajectory for that MedPac report. They do not see the impact of either program on actual people to be part of their role in advising Congress about Medicare issues.
In fact, they actually tend to complain every year that the vision benefits, hearing benefits, and dental benefits that are made available to everyone and that are appreciated most deeply by our lower income people and that happen only through the plans should not exist as benefits. The MedPac team usually says with a negative perspective that people’s expectations go up if they have eyeglasses and dental work and if they are able to hear and MedPac explicitly does not want to raise expectations of anyone on Medicare.
MedPac is actually consistently, explicitly and directly opposed to people having higher expectations and to better benefits for Medicare in those areas. They believe — incorrectly — that those benefits increase the overall cost of Medicare rather than actually use the Medicare cash flow more consistently and more effectively.
MedPac misses how much actually gets paid
They don’t understand, and they don’t believe, that the MA plans fund those additional benefits by making much better use of the Medicare dollar. That isn’t additional Medicare money. It results from the plans having costs that are below the average costs for fee-for-service Medicare in each area and it is possible for the plans to do so because fee-for-service Medicare buys care badly and delivers care poorly far too often with their much less competent use of the same dollar.
It actually costs less to buy care with MA . The plans have a process where they bid on what their monthly payment will be each year and the average bid is currently less than 85 percent of the average cost of paying for fee-for-service Medicare in each county.
They collect fewer Medicare dollars and they use them far better than those same dollars are used in the traditional payment approach that buys everything by the piece and literally does nothing in any intelligent way to get better value and higher leverage for the money they spend.
We know MA costs less because the bidding process is extremely transparent and open and it openly spends less to get more in plain sight.
The bids are actual bids and they result in actual payments. The MedPac sophists who argue as politicized theorists that the money that seems to be spent isn’t the actual cost because we need to revalue the dollars with a 9 percent judgment call to see what we are really spending because they are sure that a 9 percent inflation factor needs to be in the calculation even if it isn’t in the cash flow.
It’s a little like the old Marx movie that has MedPac saying: Who are you going to believe, me or your own eyes?
Believe your own eyes.
The bids in about a quarter of the counties fall below 80 percent of the average fee-for-service cost for each county — and stay there each year. When we look at how much we pay for each member, the actual dollars per member that is spent follow the bids — and the actual dollars go down compared to fee-for-service averages in almost all of those areas.
We don’t need to look at projections or estimates or theories on the cost of MA to figure out whether we are paying more or less. We can look at how much we actually pay and add up the dollars.
When plans bid 5 percent less and are paid 5 percent less than we can think of their costs as being 5 percent less.
MedPac does a report every year that contends that the actual amount we pay isn’t the important number for us to understand and we need to do some other calculations to see what the relative numbers actually are.
One report they do every year that distorts the relative cost of MA compared to fee-for-service Medicare looks at the actual care given to MA members and then prices that care using the Medicare fee schedule.
They look at MA enrollees and they look at their exact pattern of care and then they price that care using the Medicare fee-for-service fee schedule. They then compare that number with the capitation paid to the plans for those people and show that the numbers are consistently very different every year.
Using that model — and not adjusting it for the actual change in patterns of care — it generally looks like it costs about 4 percent more to pay the capitation than it costs to buy care for those people by the piece.
They love doing that report. It’s in this year’s annual report three times. The reality is that the care is far better for the MA plans and that’s the pattern of better care that gets priced by that process. The relevant numbers are all consistent and obvious.
MA has about 35 percent fewer emergency room days. That’s true every year. MA has programs to reduce the crisis level congestive heart failure events and that tends to result in 40 percent fewer hospital days for those patients. MA plans have many more eVisits. Fee-for-service Medicare does not pay for eVisits.
When MedPac does that cost comparison every year, they don’t have those emergency room visits in their care pattern, and that means that it looks like fee-for-service Medicare would have spent less on those exact patients.
They actually call that the overpayment report — and it typically shows that the Medicare would have spent about 4 percent less on those patients if the only care-related cash flow in their lives was the benefits that were included in the limited and standard traditional Medicare fee schedule and purchased by the piece for those exact patients.
It’s important for them to use the exact patients for that calculation, because when you use any other measurement, MA costs less. The capitation is lower than the average cost of care in all of those counties. That is extremely visible as an expense.
The plans each look at the average cost of fee-for-service Medicare in each county, and they get a chance to bid each year against those average costs and they always bid much less. In the highest cost counties for fee-for-service, even this year’s MedPac report shows that many MA plans are bidding 40 percent less.
The actual capitation that is paid to the plans each month is legitimately based on the actual average cost of care for fee-for-service Medicare in every county. That is a good, useful and important number and when we are looking at how much we are spending on each program, that average number is a very legitimate benchmark for figuring out if we are getting a good deal financially for the program.
They actually label that the benchmark process and it creates the benchmark prices that are used for enrollees in each county.
The capitation money the plans are paid each month is used by the plans to provide care, and the plans can be very flexible in how they use that money. The plans have to provide the basic set of Medicare benefits and they also need to do some defined and expected levels of quality and service reporting for that money, but they can use it in very flexible ways to provide care to their members.
They can use that money to provide additional levels of care and they can also use any and all legal caregivers available to them to serve their members in the process. A MA plan might send a nurse into a home to help with a diabetic patient or to help avert a potential congestive heart failure crisis, and they can pay that nurse to provide that care from the capitation paid to the plans. Fee-for-service Medicare does not pay for those nurses or for those sites of care — and fee-for-service Medicare would even accuse, charge and possibly indict that nurse for Medicare billing fraud if the nurse performed those same services and then sent a bill to Medicare for their time and efforts.
Quality Reporting in MA vs FFS
So MA patients tend to have both better care and more flexible care at several levels compared to fee-for-service Medicare patients. The plans also have quality reporting and expectations that do not exist at any level today in fee-for-service Medicare and that makes the MedPac comment in the report about the quality differences being completely non-discernable are discernably wrong.
We know from the current five-star reporting system that MA plans increased the percentage of cardiovascular patients who were receiving and using their statins from 80 percent to 83 percent even under Covid situations last year — and we know that the diabetics in MA plans lost ground on having their blood sugar controlled and the MA plans, on average, had that number with blood sugar controlled drop from 80 percent to 76 percent of the diabetic patients under the Covid year.
So, even though the plans did far better than fee-for-service Medicare in responding to the immediate care needs of their Covid patients, we know that they lost some ground on some levels of care during that time.
Fee-for-service Medicare, by contrast, actually does not have one single quality measure.
None.
Fee-for-service Medicare simply does not do any quality improvement programs. They also don’t set any quality goals, and fee-for-service Medicare does not support or pay for team care or for medical information pooling and linkages for their patients for use in care quality activities for their caregivers.
The MedPac staff wrote again in their report about the status of MA that they could not comment on the quality of care in fee-for-service Medicare compared to MA because they have no data for those fee-based patients, which means that it is impossible and wrong for MedPac to comment on the comparative quality of care. They believe and they say that clear deficit in quality data that exists for fee-for-service care sites and those caregivers should not cause anyone to conclude anything about the relative quality of the two programs, or should be a reflection in any way on any part of the fee-for-service Medicare, because that would be “unfair to fee-for-service Medicare” to point that data issue out in any public way.
That avoidance of the quality issue is just wrong.
I’ve given DNA a lot of love over the years — DNA as a storage medium, as a computing platform, as the basis for robots, as the tool for synthetic biology/biohacking, even used for the DNA-of-Things (DoT). DNA is the basis for all life as we know it, in every category of life we’ve found anywhere on earth. That we are now using it to achieve technological goals seems like one of humankind’s greatest accomplishments.
But where’s the love for RNA, DNA’s putative ancestor and still-partner? A few recent developments in RNA caught my eye that I wanted to give their due.
As you may remember from high school biology, RNA has a crucial role in how DNA transmits genetic information. As one source explains it: “DNA holds information, but it generally does not actively apply that information. DNA does not make things.” Instead, it transcribes the information onto RNA, which then actually makes things happen.
Just last week researchers from Northwestern University were able to show RNA switching genes off and on, using a simulation model they “affectionately” call R2D2 (short for “reconstructing RNA dynamics from data”). The researchers believe the “strand displacement” mechanism is what switches genes “on” or “off.”
Professor Julius B. Lucks, who co-led the research, believes: “Many diseases are likely caused by something going awry at the RNA level. The more we know about this, the better we can design RNA targeting drugs and RNA therapeutics.” For example, genes could be “engineered to turn “on” in the presence of an environmental contaminant.”
Amazing stuff. But that’s not all.
Researchers at the University of Tokyo have created an RNA molecule that can not just replicate but evolve. There has long been a hypothesis, called “RNA World,” which speculates that RNA is the basis for the origin of life, with DNA coming along at some later point (DNA is believed not to be stable enough to survive, much less evolve, in the primordial environment). The research makes that hypothesis even more plausible.
The team seeded an RNA molecule, which evolved into several lineages before stabilizing: “The final population, comprising five RNA lineages, forms a replicator network with diverse interactions, including cooperation to help the replication of all other members.”
The results were somewhat surprising, even to the researchers. “Honestly, we initially doubted that such diverse RNAs could evolve and coexist,” said Ryo Mizuuchi, corresponding author of the study.
We will probably never know how life on earth actually emerged, but the researchers claim:
Our results demonstrate an evolutionary transition scenario of molecular replicators from a single common ancestor to a multi-membered network…Thus, our simple experimental setup offers a unique approach to deeply look into evolutionary phenomena.
OK, that’s two long-time mysteries answered, or at least addressed, by RNA. Here’s an even more fun one: RNA computers.
There has been discussion of DNA computers for many years. However, as NIST (National Institute of Standards and Technology) says:
Tiny biological computers made of DNA could revolutionize the way we diagnose and treat a slew of diseases, once the technology is fully fleshed out. However, a major stumbling block for these DNA-based devices, which can operate in both cells and liquid solutions, has been how short-lived they are. Just one use and the computers are spent.
Instead, in a new paper, NIST researchers used RNA to build computers. Or, more precisely:
Here, we develop scalable cotranscriptionally encoded RNA strand displacement (ctRSD) circuits that are rationally programmed via base pairing interactions. ctRSD circuits address the limitations of DNA-based strand displacement circuits by isothermally producing circuit components via transcription.
Samuel Schaffter, the lead author and a NIST postdoc researcher, explained how DNA and RNA computing differs from typical computing: “The difference is, instead of coding with ones and zeroes, you write strings of A, T, C and G, which are the four chemical bases that make up DNA.” The authors tested whether the RNA-based circuits could perform logical operations (I won’t even attempt to describe exactly how they did this).
Dr. Schaffter said: “For me, these needed to work in a test tube as predictively as DNA computing. The nice thing with DNA circuits is most of the time, you can just write out a sequence on a piece of paper, and it’ll work the way you want. The key thing here is that we did find the RNA circuits were very predictable and programmable, much more so than I thought they would be, actually.”
The authors are quite excited about future applications. E.g., “We envision ctRSD circuits enabling many new applications in nucleic acid computing and synthetic biology. For example, the inclusion of ribonucleases in ctRSD circuits would allow continuous circuit turnover. Circuits could then respond multiple times to changing input signals, overcoming a current challenge in DNA computing.”
As for the next step, Dr. Schaffter sees: “We’re interested in putting these in bacteria next. We want to know: Can we package circuit designs into genetic material using our strategy? Can we get the same sort of performance and behavior when the circuits are inside cells? We have the potential to.”
I can’t wait for Raspberry Pi to come out with their RNA-based computer. You watch.
————-
All this sounds very esoteric and perhaps not applicable to the immediate woes of our healthcare system, but I’m thinking about the rest of the 21st century and beyond. As I’ve said before, the 20th century may have been the age of computers, but the 21st century is going to be the age of biology.
If we believe that the 20th century ushered in “modern medicine,” with more rigorously trained professionals using more scientific tools (think antibiotics, imaging, laparoscopic surgeries, A.I., etc.), then 21st century healthcare is going to be about synthetic biology. Thinking about DNA and RNA isn’t going to just be something healthcare professionals do to satisfy their undergraduate requirements; it’s going to be integral to their toolset.
What’s going to be very interesting – and highly disruptive — is not just how this change will impact our health and our healthcare, but also what happens to physicians, nurses, pharmacies in a world where biologists/biochemists/geneticists may play the more important role.
Kim is a former emarketing exec at a major Blues plan, editor of the late & lamented Tincture.io, and now regular THCB contributor.
Each week I’ve been adding a brief tidbits section to the THCB Reader, our weekly newsletter that summarizes the best of THCB that week (Sign up here!). Then I had the brainwave to add them to the blog. They’re short and usually not too sweet! –Matthew Holt
For my health care tidbits this week, the controversy about Medicare Advantage is getting louder and louder. There’s no question that it results in lower out of pocket payments for its members than traditional FFS Medicare. Medicare Advantage members use fewer services, and their care appears to be better “managed” –then again FFS Medicare’s “members” are barely managed at all.
But the big question is, Does Medicare Advantage save the government money? Critics (notably ex CMS veterans Berwick & Gilfillan) claim that risk adjustment games played by the private plans who run Medicare Advantage have cost up to $200bn over 10 years. Medpac (the independent body that advises Congress) estimates that “Medicare spends 4 percent more for MA enrollees than it would have spent if those enrollees remained in FFS Medicare” and go on to say “In aggregate, for the entire duration of their Medicare participation, private plans have never produced savings for Medicare”. However data from the Medicare Trustees and other research from ACHP & the trade group Better Medicare Alliance suggests that Medpac’s analysis is incorrect and that Medicare Advantage saves the government about 9% per enrollee.
THCB ran a long piece (pt 1, pt 2) about Medicare Advantage from former Kaiser Permanente CEO George Halvorson earlier this year, and a related one from current Permanente Federation CEO Richard Isaacs. But it’s much more nuanced than that. J Michael McWilliams has long piece on Health Affairs Forefront trying to capture the various strands of the argument. His conclusion? “The substantial subsidies MA receives are largely responsible for the extra benefits and have more than offset savings from any efficiencies, posing a net cost to Medicare and complicating assessments of MA’s added value.”
Meanwhile CMS has just changed the most controversial aspect of risk adjustment (which is the most controversial part of Medicare Advantage) by banning the plans from doing it, and only allowing providers to be involved.
Whether any of this is going to change CMS regulations or wider government policy regarding MA payments is less certain. CMS is currently dealing with its replacement for the even more controversial Direct Contracting (now called ACO REACH). But Medicare Advantage is the most profitable part of private health insurance and has many knock on effects for care services and technology. So I’ll be watching this space and you should too!
Matthew Holt categorized the triple-merger between Cricket Health, Fresenius Health Partners, and InterWell Health as a “take out merger” — proposing that Fresenius orchestrated the deal to “take out” rising-star kidney care startup, Cricket Health. Well, Cricket Health’s CEO Bobby Sepucha (who will also be CEO of the newly combined entity) “takes issue” with the health tech curmudgeon’s “take out” call and we find out the reasons why.
Listening to Bobby’s explanation, it sounds like the shrewd move Fresenius might be making here in giving up its value-based care arm, Fresenius Health Partners, and its joint-venture with 600 nephrologists in InterWell Health is one that better positions their core dialysis business for the value-based care future that is headed straight toward specialty medicine.
As Bobby puts it, “when you deliver a healthier patient to kidney failure, you don’t obviate the need for dialysis.” Instead, he says, you open up options for other treatments like transplant or home dialysis along the way, as well as the kinds of patient quality outcomes that satisfy the clinical accountability of providers in value-based arrangements.
The other gain is a move upstream for Fresenius. While there are 600,000 dialysis patients each year, the population of Americans with late-stage kidney disease who remain “wildly unmanaged” is 36 MILLION. And they represent $170 Billion in healthcare costs. If InterWell works the way it’s supposed to – with the first value-based care-designed model for late-stage kidney disease management – the potential to impact that patient population is what this merger is all about. Tune in and tell us what you think!
Recently, despite decades of experience in cybersecurity, privacy, and data science, I got sent back to school.
As a member of the Council of the Wise at the Light Collective, a patient advocacy group with a focus on healthcare technology and privacy, I attended a town hall event entitled “No Aggregation Without Representation,” which featured four eminently qualified leaders of the BIPOC and data advocacy communities: Dr Maya Rockeymore Cummings, Tiah Tomlin-Harris, Jillian Simmons, JD and Valencia Robinson. I was unprepared for the ownership and authority of these four leaders – and unprepared, too, for how they were able to transform professional truisms I’ve often relayed myself into something far more personal, meaningful, urgent, and authentic.
The commercial practice of aggregating health and consumer data crosses the borders of healthcare, retail, marketing, communications, transportation, and others. The risks and consequences (including abuse) related to the exploitation and monetization of personal health data are enormous, complex, and largely or entirely borne by the individuals whose data is being collected – whether they know it or not.
What’s more, none of the current patchworks of 3-letter federal regulatory bodies (FDA, FTC, HHS, FCC) have the remit or resources to encompass the totality of it. Armed with pre-Internet privacy laws from the 1970s or with insurance portability laws from the mid-1990s that have been stretched to cover health and consumer privacy protections, a constellation of advocacy organizations, ethicists, and academics identify problems and offer opinions. All the while, though, data flows like oil to fuel a surveillance economy in which consumers and patients are exploited and harmed. For vulnerable communities including BIPOC and persons with frailties, disabilities, or mental illness, these harms are not only real, but – in light of sad history – they are also unsurprising.
The Deep Roots of Systemic Harm
During the town hall, the panelists describe an ongoing lack of trust that has grown steadily from events such as the Tuskegee syphilis experiments that began in the early 1930s and continued up until the early 1970s, the case of tissues taken without consent or compensation from Henrietta Lacks in the 1950s and used in thousands of experiments, and the continued stigma surrounding diseases such as HIV that are no less potent today than they were in the 1980s. As I listened to the panelists, these events were no longer historical to me, but instead were current events unfolding before my eyes and deeply affecting communities who are well aware that they are being harmed and exploited so that others may profit.
But just what are those harms, and who feels their effects? Those who pontificate about the virtues and value of data without boundaries often argue that the benefit to the many outweigh the risks to the few, but it is not “just a few” when we are talking about significant numbers of individuals within minority and underserved communities. In the last few weeks alone, we have read stories about how data from persons seeking help due to suicidal ideation was captured and monetized by a crisis text line, seen credible evidence of how middleware ad tracking software can track users regardless of stated privacy policies on some health sites, and witnessed another class-action lawsuit against Meta (Facebook’s parent company) for the misuse of personal biometric data.
Patient populations need rights. So what?
I once had a mentor who advised me to ask myself, “so what?” at least three times before deciding whether an idea could stick. Let’s play that game using the wisdom shared by these four amazing leaders…
Dr. Rockeymore Cummings spoke about how she had shared parts of her health journey story online to provide support to others on similar journeys. But the ultimate outcome of this sharing was that her insurance company asserted that because she had advocated for preventative options, the procedures she had undergone were elective, and therefore denied coverage for them. Where is the internet warning label that advises consumers that the thoughts and experiences they share online may be scraped, scrutinized, and interpreted by their health insurance companies? Interestingly, when the human genome was first mapped, scientists and ethicists helped ensure the passage of the Genetic Information Nondiscrimination Act (GINA) because they foresaw the potential for abuse when information about individuals’ genetic makeups became available. But over the decades that the internet has been proliferating, no comparable nondiscrimination protections have emerged to cover the myriad other kinds of personal data available online. To surveillance capitalists, this situation is a feature, not a bug.
Patient populations’ data are owned by companies. So what?
Today we live in a world where any given patient population’s collective health data is owned by companies. And what we share is increasingly part of our permanent public record. So what? What if I did say something like that once, and I changed my mind? Or what if I signed up for a service that required some of my data but then decided I was no longer interested, or worse, was worried about things I learned as I became more familiar with the service? Jillian Simons pointed out that not a single state has passed comprehensive “right to be forgotten” privacy protections, which would grant people the right to have their personal data removed from specific and aggregated datasets. Beyond the obvious assurances, this approach affords to patients and consumers, it’s also an extremely effective way to ensure accountable stewardship of data, even in large, aggregated datasets. The right to be forgotten imposes a duty on the dataset owner/aggregator to know where that individual‘s data resides and where it has been shared; otherwise, their data cannot be found to be erased if they so desire. As they would say in my hometown of Boston, “wicked smaht.”
So what?
If experiencing denial of care or preserving personal autonomy about participating in health websites are not sufficiently compelling issues, let’s get to the tougher stuff. As our preprint article (recently covered by Wired magazine) shows, health sites are using – sometimes without even realizing it – middleware that contains ad trackers. Ad tracking may not seem like something that’s obviously harmful, but such trackers can aggregate strikingly personal information from seemingly benign data. For instance, if you’ve used a ride-sharing app, your physical location might be shared across multiple platforms. Use that ride-sharing platform to visit Planned Parenthood, and various inferences could be drawn. Data from multiple browser windows left open on your phone can be aggregated to know your online purchases, the stores you frequent, the banking tools you use, the restaurants you visit – or when you’re at home waiting for a pizza. At this point, the question of “so what” should be thoroughly answered. Does all of this still sound benign?
Real World Data: Meet the Real-World Hazards
Pharma and digital health companies often tout the benefits of real-world data to improve population health. These data hold power to create huge advancements in our understanding of disease. We need real world data. Yet without proper protections and stewardship, these data hold hazards, and are left unprotected. All of these data and more are being grabbed by stalker were that is proliferating in epidemic proportions, and vulnerable people are most affected. One study in the European Institute for Gender Equality found that 7 out of 10 women in Europe that had experienced cyberstalking were also victims of intimate partner violence. According to this report, the digital control exercised by a stalker can be immense: reading anything the surveilled person types, including user names and passwords for services such as banking applications, online shops and social networks; knowing where that person is by tracking their movements in real time with GPS; eavesdropping on or even recording phone calls, or even record them; reading text messages (regardless of whether encryption is used); monitoring social network activity; viewing photos and videos; and even being able to switch on the camera.
Another survey showed that 85% of domestic violence workers reported having cared for victims whose attacker located them by GPS. Further, the statistics on the adverse effects of internet crime on racial and ethnic minorities show that BIPOC communities face identity theft more often, that the social media accounts of BIPOC communities are attacked more often, and that elderly persons are targeted more often than those under 65. Put simply: the more vulnerable are more vulnerable.
So why do we say “no aggregation without representation?” It’s not an abstract ethical question about privacy or even autonomy. It is the right to be safe. The right to feel secure. That makes it no less than a civil right.
This concept of collective rights, representation, and stewardship of real-world health data is only getting started. Those of us in healthcare who hold power, privilege, and influence have a responsibility to listen and act. So what comes next?
Exciting things are a-happening in the Medicaid space! Two new female CEOs are being announced today in City Block Health and in Centene! In this episode of Health Tech Deals, Jess and I discuss new leadership changes in the health tech space, as well as new deals: Huma buys Astra Zeneca Digital; Afterlife raises $22 million; Timedoc Health raises $48.5 million; Avive raises $22 million; Antidote Health raises $22 million.
Joining Matthew Holt (@boltyboy) on #THCBGang at 1pm PT 4pm ET Thursday for an hour of topical and sometime combative conversation on what’s happening in health care and beyond will be: Queen of all employer benefits Jennifer Benz (@Jenbenz); fierce patient activist Casey Quinlan (@MightyCasey); patient safety expert and all around wit Michael Millenson (@MLMillenson); THCB regular writer and ponderer of odd juxtapositions Kim Bellard (@kimbbellard); and back from his travels in Mexico and medical historian Mike Magee (@drmikemagee).
Special guest this week is population health and primary care expert Ines Vigil, who developed that program at Johns Hopkins but now hangs her hat at Clarify Health & author of Population Health Analytics.
You can see the video below live (and later archived) & if you’d rather listen than watch, the audio is preserved as a weekly podcast available on our iTunes & Spotify channels.